In this post, I link to and excerpt from Diagnosis and Management of Transient Ischemic Attack, Continuum (Minneap Minn). 2017 Feb;23(1, Cerebrovascular Disease):82-92 [PubMed Abstract] [Full-Text HTML] [Full-Text PDF] from The American Academy of Neurology.
There are 25 similar articles from 2017 through today’s date in PubMed Central.
The above article has been cited by 16 articles in PubMedCentral.
All that follows is from the above resource.
KEY POINTS
Abstract
Purpose of review: This article reviews the diagnosis, investigation, and recommended management after a transient ischemic attack (TIA) and discusses how to make an accurate diagnosis, including the diagnosis of mimics of TIAs.
Recent findings: Up to a 10% risk of recurrent stroke exists after a TIA, and up to 80% of this risk is preventable with urgent assessment and treatment. Imaging of the brain and intracranial and extracranial blood vessels using CT, CT angiography, carotid Doppler ultrasound, and MRI is an important part of the diagnostic assessment. Treatment options include anticoagulation for atrial fibrillation, carotid revascularization for symptomatic carotid artery stenosis, antiplatelet therapy, and vascular risk factor reduction strategies.
Summary: TIA offers the greatest opportunity to prevent stroke that physicians encounter. A TIA should be treated as a medical emergency, as up to 80% of strokes after TIA are preventable.
INTRODUCTION
Transient ischemic attack (TIA) and minor ischemic stroke are associated with brain dysfunction in a circumscribed area caused by a regional reduction in blood flow (ie, ischemia), resulting in either transient or minor observable clinical symptoms. Identification of ischemia is important as 20% of patients with ischemic stroke present with a TIA in the hours to days preceding the stroke.1,2 Up to 80% of strokes after TIA are preventable; thus, early diagnosis and treatment are key.
DEFINITION AND CLINICAL DIAGNOSIS
The clinical definitions of TIA and ischemic stroke are based on focal neurologic signs or symptoms referable to known cerebral arterial distributions without direct measurement of blood flow or cerebral infarction. It is important to note that TIA and stroke represent different ends of an ischemic continuum from the physiologic perspective, but clinical management is similar. The historical time-based definition of TIA was based on full resolution of all symptoms within 24 hours of onset. The time-based definition has been debated in light of diffusion-weighted MRI demonstrating relevant ischemic lesions in 30% to 50% of patients fulfilling the time-based definition of TIA (Case 4-1).3,4 It is also relevant that the diagnoses of TIA and minor stroke are commonly used interchangeably and recorded as such in medical records. Although this article focuses primarily on TIA, a significant difference in the outcome of TIA compared to minor ischemic stroke has not been demonstrated by compelling evidence. Treatment to prevent ischemic stroke following TIA and treatment to prevent recurrent stroke following minor ischemic stroke are also similar. Very early assessment of these patients also makes the distinction between TIA and minor ischemic stroke difficult.
The diagnosis of TIA depends on the quality and quantity of information available and the time of assessment. The main criteria used are the clinical history or objective findings on neurologic examination consistent with focal neurologic dysfunction at some point of the evaluation and imaging of the brain. A limitation of the clinical definitions of stroke and TIA is that they rely on the presumed cause of the symptoms: ischemia. Symptoms are attributed to ischemia based mainly on the time course of the deficits (an acute deficit is more consistent with ischemia), the distribution of the deficits, and background risk factors for ischemia in the patient. Because patients vary in reliability in reporting the events they have experienced, even an astute physician may find it challenging to make a certain diagnosis based on the history and physical examination alone. Even experts do not agree about which clinical events are in fact TIAs.5–7
One of the problems with assessment is that half of all patients presenting to emergency departments and physicians’ offices in North America with transient or mild neurologic deficits have symptoms with an uncertain diagnosis or prognosis. Some have, indeed, had an ischemic event, but others have had symptoms related to a stroke or TIA mimic, such as migraine, epilepsy, multiple sclerosis, or peripheral nerve entrapment (Case 4-2). The prevalence of these mimics is higher among clinical presentations without motor and speech symptoms. Motor and speech symptoms may have a higher likelihood of brain ischemia as the cause of the symptoms because the differential diagnosis for such clinical presentations is much narrower, and patients who present with motor or speech symptoms are known to be at high risk for recurrent stroke.8 However, patients who present with symptoms other than motor and speech symptoms (eg, sensory symptoms or dizziness) have a more uncertain etiology.9 This is likely related to the higher probability of a nonischemic cause of symptoms in these patients. Posterior circulation ischemia can pose an additional diagnostic challenge as symptoms are more variable than those that occur with hemispheric ischemia.10 Although the proportion of patients with true ischemia is lower in those without motor or speech symptoms, it is important not to miss patients with true TIAs and minor ischemic strokes.10,11
Case 4-1
A 57-year-old man presented with a 2-minute episode of left hand weakness. During the episode, his left hand became unusable and he could not pick anything up; he was able to lift his arm, although it felt weak. He was able to walk and talk normally throughout the episode. On presentation to the emergency department, he was completely back to normal. Head CT and CT angiogram were normal. However, the diffusion-weighted MRI showed a small lesion in the right hemisphere consistent with his symptoms (Figure 4-1).
Comment. This case illustrates that transient neurologic symptoms can be associated with evidence of ischemia on diffusion-weighted brain MRI sequences. As many as 50% of patients clinically diagnosed with a transient ischemic attack using a time-based definition have evidence of restricted diffusion on an acute MRI scan.
Case 4-2
A 75-year-old man presented to the emergency department after experiencing a 10-minute episode of right hand weakness 2 hours earlier, after which he completely returned to normal. He had no significant past medical history and was on no medications. Neurologic examination was normal. Urgent brain CT showed a left-sided chronic subdural hematoma. He was referred for neurosurgical assessment.
Comment. Many different mimics of transient ischemic attack exist, as in this case. Hemorrhage is a rare, but important, cause of transient neurologic symptoms. This case highlights the recommendation that all patients with transient neurologic symptoms should have brain imaging not only to look for ischemia but also to look for other causes of transient neurologic symptoms. It also emphasizes the fact that clinically one cannot reliably diagnose brain hemorrhage; brain imaging is necessary to differentiate between ischemia and hemorrhage. Subdural hematomas are common in the elderly and may occur spontaneously without a history of trauma. The mechanism behind why subdural hematomas can present with transient neurologic symptoms is not entirely clear, but theories include mechanical compression of vessels, partial seizures, or spreading cortical depression.
TAKING A HISTORY FROM A PATIENT WITH A POSSIBLE TRANSIENT ISCHEMIC ATTACK
The diagnosis of TIA remains largely clinical and is based on taking an accurate history. This contributes to the variability in the diagnosis of TIA, with high rates of disagreement seen even between neurologists.5 As many as 60% of patients referred to a TIA clinic will not have a final diagnosis of TIA.12,13 Identification of possible TIA mimics is an important stage in the assessment of patients with transient neurologic symptoms. An accurate diagnosis of a stroke mimic impacts treatment decisions and provides reassurance when the diagnosis is something more benign than TIA.
The clinical history is most accurate when taken close to the resolution of the event. Accuracy is also best when the patient first reports symptoms compared to the history obtained after the patient has provided multiple iterations to medical personnel.
A TIA is a clinical syndrome characterized by the sudden onset of a focal neurologic deficit presumed to be on a vascular basis. As the definition implies, key points of the history need to be elicited from the patient. Imaging can support the diagnosis, but TIA is primarily a clinical diagnosis. Descriptors such as “numb,” “dead,” “heavy,” or “weak” may have different meanings for different patients and require clarification, similar to the different meanings patients may have for “dizzy.” The most important clinical determination is whether the neurologic symptoms are focal or nonfocal. Regional cerebral ischemia causes focal symptoms. Focal neurologic symptoms usually affect one side of the body (eg, weakness or sensory abnormality on the right or left side). Nonfocal neurologic symptoms include generalized weakness, light-headedness, fainting, blackouts, and bladder or bowel symptoms. Although patients with the nonfocal symptoms of syncope or presyncope are sometimes referred for assessment of possible TIA, loss of consciousness is only very rarely a symptom of stroke or TIA.
INVESTIGATIONS
A full neurologic and cardiac examination should be completed on all patients with suspected TIA. Blood pressure, pulse rate, and oxygen saturation should be obtained, and an ECG should be performed to evaluate for atrial fibrillation. Many patients will also require an echocardiogram and some form of extended cardiac monitoring if no definitive cause is found for the TIA. For more information about assessment for a cardiac source of emboli, refer to the article “Cardioembolic Stroke” by Cumara B. O’Carroll, MD, MPH, and Kevin M. Barrett, MD, MSc,14 in this issue of Continuum.
Routine blood work should also be completed on all patients, including:

Fasting lipids and glucose need to be assessed as well, but these are often obtained after the first visit. Although most patients will have a single diagnosis, diagnostic tests such as ECG and oxygen saturation can be useful to identify the occasional patient who has two concurrent diagnoses, such as TIA and pulmonary embolus or a myocardial infarction.
PROGNOSIS
About 10% of patients presenting with TIAs or minor strokes will have a stroke within the next 90 days,8,15,16 with the highest risk period being the first 24 hours.17 Wide consensus exists that TIA and minor ischemic stroke are medical emergencies that necessitate immediate management.18
Clinical/Event Features and Score
The ABCD2 score has emphasized that taking a detailed history is important, and it has raised awareness within the general medical community that recognizing TIA is an important way of preventing stroke. However, the problem with the ABCD2 score is that patients in the low-risk category still have recurrent strokes.22 Also, in terms of absolute numbers, the majority of recurrent strokes are in the moderate category. Some patients who are classified as having low risk on the ABCD2 score may have important potentially treatable TIA etiologies, such as symptomatic carotid artery stenosis or atrial fibrillation, that require urgent treatment.23 These limitations have prevented widespread adoption of the ABCD2 score to triage patients with TIA.24
The Rotterdam Study25 followed patients with transient neurologic attacks for 10 years and found an increased risk of stroke not only in patients with focal symptoms (ie, possible TIAs) but also in patients who had transient episodes of nonspecific symptoms. It is likely that these patients represent a heterogeneous group with variable risk of recurrent stroke. It is therefore timely for the neurologic community to progress beyond the ABCD2 score to improve our ability to define the clinical outcome of patients on an individual basis. Posterior circulation events, in particular, can cause nonspecific symptoms.26
Imaging and Prognosis
Evidence of an acute infarct on a noncontrast CT alone has been shown to be predictive of recurrent stroke in patients with TIA (ie, patients whose symptoms had resolved), although the proportion of patients with evidence of acute infarcts was small (4%).27 Patients with minor ischemic stroke and TIA who are at the highest risk of recurrent events and disability can be identified using noninvasive CT angiography (CTA).28 CTA is a quick and easy addition to the noncontrast CT that is completed on most patients and provides much more information than a noncontrast CT alone, with imaging of the intracranial and extracranial vessels. The addition of better imaging techniques, such as multiphase CTA and CT perfusion, provides the ability to identify more distal occlusions than previously. Evidence of 50% or greater stenosis or occlusion in a symptom-relevant vessel in the intracranial or extracranial circulation puts a patient at high risk of a recurrent stroke.28 Understanding the pathophysiology of a TIA or minor ischemic stroke is paramount to preventing recurrent stroke. Using CT/CTA to assess patients in the emergency department has allowed many patients to be safely triaged, with patients with abnormal CT/CTA admitted for observation and those with normal imaging being assessed as outpatients.29 Other modalities for imaging cervicocephalic vessels, such as magnetic resonance angiography (MRA), are also acceptable. Carotid duplex ultrasound is an additional noninvasive modality commonly used to evaluate for hemodynamically significant carotid occlusive disease at the bifurcation. Identification of high-grade stenosis in the carotid artery ipsilateral to retinal or hemispheric symptoms may be indicative of stroke mechanism and near-term stroke risk. Carotid ultrasound does not adequately evaluate the carotid circulation beyond the bifurcation (ie, distal cervical and intracranial segments), and additional vascular imaging modalities may be necessary when the index of clinical suspicion is high for vertebrobasilar or intracranial occlusive disease.
Brain imaging using MRI is a very sensitive way of assessing for brain ischemia. Diffusion-weighted imaging (DWI), which shows the abnormal diffusion of water in the setting of focal brain ischemia, is the most helpful sequence. Up to 50% of patients clinically diagnosed with a TIA using a time-based definition have evidence of restricted diffusion on an acute MRI scan. Most studies of recurrent stroke after TIA have shown an increased risk of short-term recurrent stroke in the presence of a lesion seen on DWI. However, the exact magnitude of the risk depends on the population studied. Whether the presence or absence of a lesion on DWI changes the longer-term (1- to 5-year) risk of stroke is less clear. The lesion pattern on an MRI can change the vascular localization in up to one-third of patients. Infarct topography can also be useful to inform stroke mechanism (eg, involvement of more than one vascular territory being suspicious for a proximal embolic source such as atrial fibrillation).
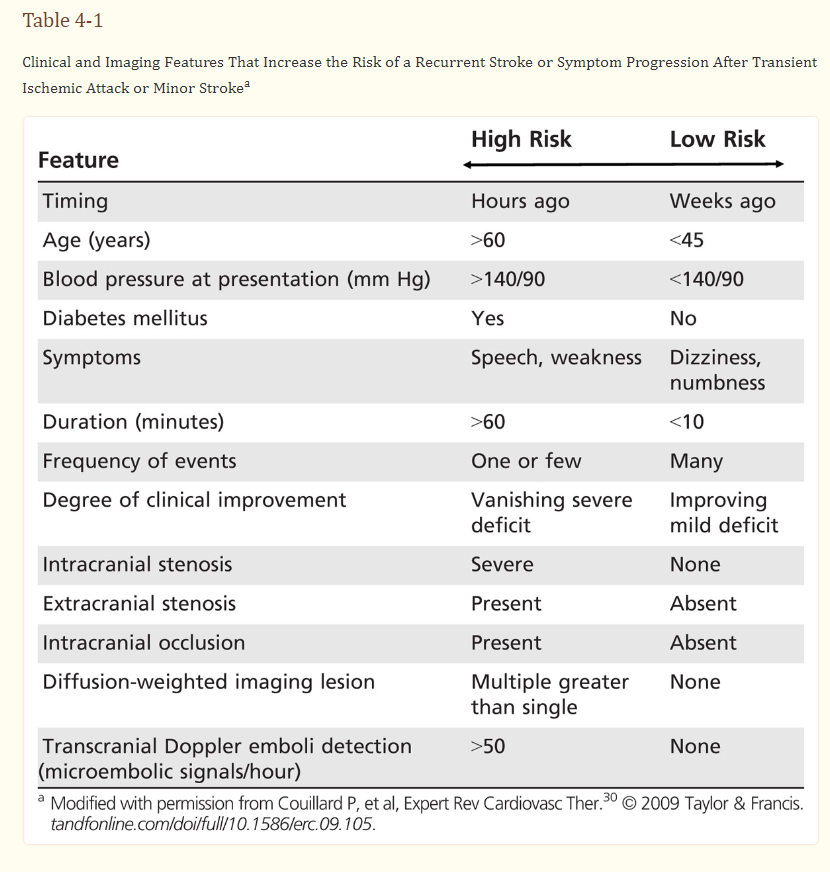
Many stroke neurologists find MRI particularly helpful in cases in which the diagnosis is not 100% clear based on the history. MRI results must always be taken in the appropriate clinical context. Most stroke neurologists would agree that patients who have a negative DWI but have truly had TIAs clearly exist, and thus they will treat patients for TIA even with a negative DWI. There has been some discussion over the past few years about calling transient symptoms a clinical TIA, but calling symptoms in combination with a lesion seen on DWI a stroke. From a practical perspective, it does not matter what it is called; what is important is that patients get the appropriate early assessment and treatment (Table 4-130)
TREATMENT
Recognition and management of TIA offers the greatest opportunity to prevent disabling stroke. Studies have shown up to an 80% reduction in the risk of stroke after TIA with the early implementation of secondary stroke prevention strategies,11,12 including revascularization of patients with symptomatic carotid artery stenosis, anticoagulation of patients with atrial fibrillation, treatment with antiplatelet agent(s), treatment with statins for most patients, management of hypertension, and lifestyle interventions, such as smoking cessation or weight loss.
Early carotid revascularization for patients with 50% or greater symptomatic carotid artery stenosis is an effective form of stroke prevention when performed within the first 2 weeks after an event. If a patient is stable, surgery should be performed as soon as possible (Case 4-3). It is important to identify carotid stenosis because, although it causes only 10% of all TIAs, it causes 50% of early recurrences. It is a treatable condition, and it is tragic when a recurrent stroke occurs in someone waiting for a carotid endarterectomy.
All patients with TIAs should be on an antiplatelet agent, except for those who are being anticoagulated for atrial fibrillation. For most patients, it will be a single antiplatelet agent, usually aspirin monotherapy (81 mg/d to 325 mg/d). Other options include 75 mg/d clopidogrel or a combination of 25 mg aspirin and 200 mg extended-release dipyridamole 2 times a day.29
Two randomized clinical trials have provided evidence for the short-term use of dual antiplatelet therapy after TIA and minor ischemic stroke. . . . For now, North American secondary stroke prevention guidelines do not recommend dual antiplatelet agent therapy.29*
*This article is from 2017. Thus, it would be reasonable to consult a neurologist for guidance when TIA is diagnosed.
Outpatient Versus Inpatient Assessment
For stroke prevention, the location of treatment matters less than the speed of the assessment. However, in most parts of the world, assessing patients and completing urgent (on the same day, within a few hours) imaging is most easily done in the emergency department given the easy access to imaging. In clinical settings that do not have access to timely outpatient neuroimaging, patients are often admitted to the hospital to complete TIA evaluation and expedite initiation of secondary prevention strategies. Some advantages of admitting the patient to the hospital include close neurologic monitoring and early completion of investigations and appropriate treatment.
Case 4-3
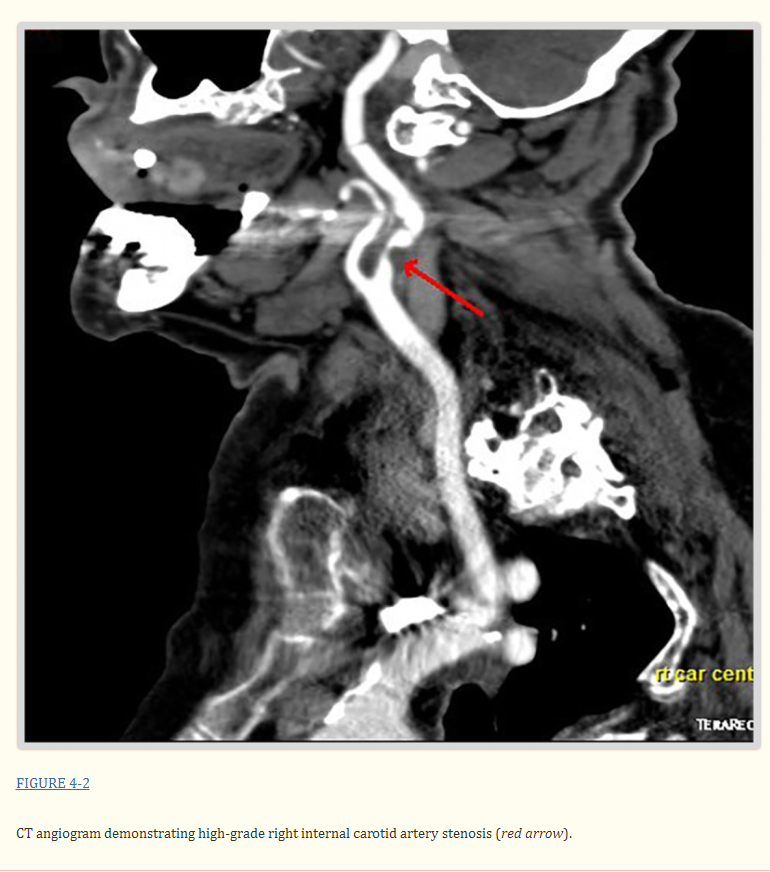
A 50-year-old man presented to the emergency department with an episode of left hemiplegia that lasted 5 minutes. He smoked cigarettes but otherwise had no significant past medical history. His examination was normal, with blood pressure of 125/75 mm Hg and an ABCD2 (age, blood pressure, clinical features, duration, presence of diabetes mellitus) score of 2. Head CT was normal, but CT angiography showed a high-grade stenosis of the right internal carotid artery (Figure 4-2). He was started on 81 mg aspirin and 40 mg of simvastatin daily. The patient underwent right carotid endarterectomy the next day without complication.
Comment. This patient had a transient ischemic attack and was at high risk of early recurrent stroke, although it was not identified as such by the ABCD2 score. Carotid artery stenosis is an important cause of a transient ischemic attack with a high risk of recurrence. Early vascular imaging is required to identify this treatable cause of stroke. Carotid revascularization should be performed as soon as reasonably possible if the patient is medically stable.
CONCLUSION
The assessment of TIA is all about making the correct diagnosis, and taking a good history is key. Once a TIA diagnosis has been made, cardiac and neurovascular imaging can help inform the potential etiology and guide initiation of evidence-based secondary stroke preventative strategies. Ideally, obtaining the history, imaging, and identifying the etiology occur on the same day as presentation to reduce the risk of recurrent cerebral ischemia.