In this post, I link to and excerpt from Serum Protein Electrophoresis. Updated: Dec 16, 2021 Author: Sherilyn Alvaran Tuazon, MD from the outstanding medical reference resource, emedicine.medscape.com.
All that follows is from the above outstanding resource.
Reference Range
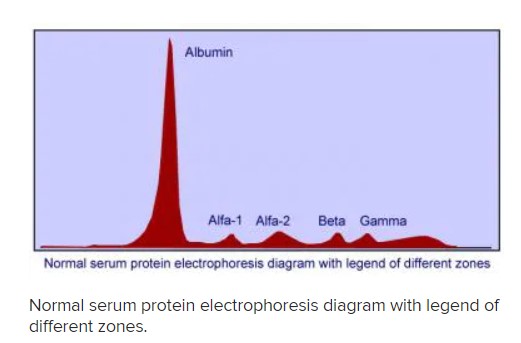
Serum protein electrophoresis (SPEP) is an easy, inexpensive method of separating proteins based on their net charge, size, and shape. The 2 major types of protein present in the serum are albumin and the globulin proteins. Albumin is the major protein component of serum and represents the largest peak that lies closest to the positive electrode. [1] Globulins make up a much smaller fraction of the total serum protein but represent the primary focus of interpretation of serum protein electrophoresis. Five globulin categories are represented: alpha-1, alpha-2, beta-1, beta-2, and gamma, with the gamma fraction being closest to the negative electrode.
Interpretation
Monoclonal gammopathy
A dense narrow band that is composed of a single class of immunoglobulins secreted by an abnormally expanded clone of plasma cells is known as M-protein (paraprotein, monoclonal protein, or M-component). [3, 4] An M-protein usually presents as a single narrow peak, resembling a “church spire,” in the gamma, beta, or alpha-2 region of the densitometer tracing, or as a dense, discrete band on the agarose gel (see image below).
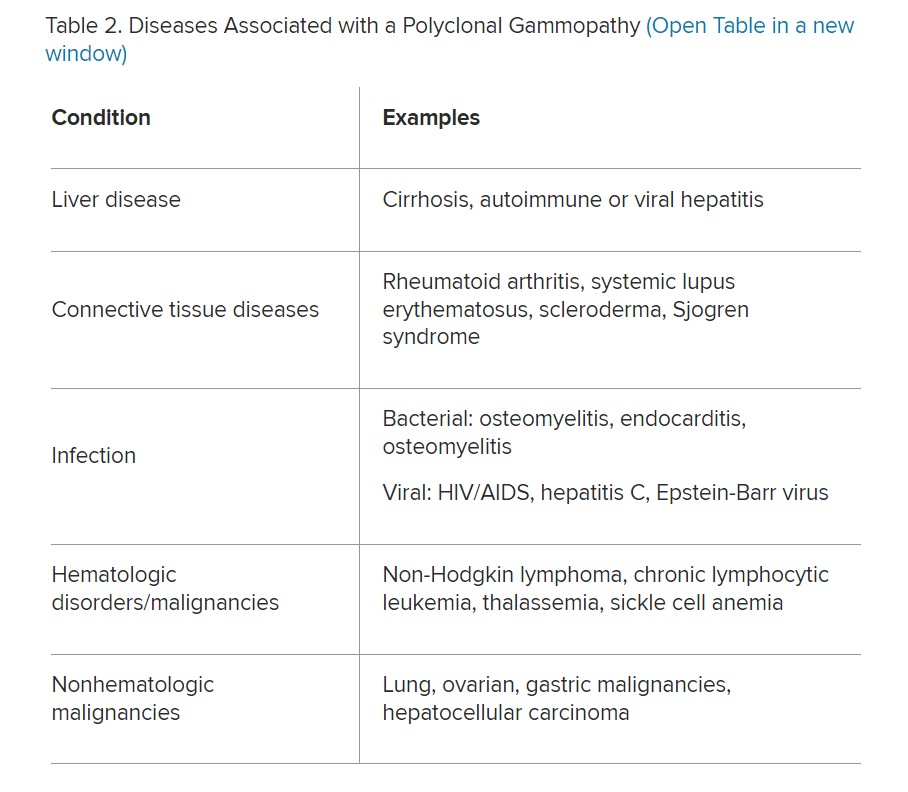
The monoclonal antibody must be present at a concentration of at least 0.5 g/dL in order to be accurately identified using SPEP. This corresponds to approximately 109 antibody-producing cells. [5] Plasma cell disorders are typically associated with the presence of an M-protein (see Table 2 below). In addition, an M component may be detected in other lymphoid malignancies like chronic lymphocytic leukemia, any B- or T- cell lymphomas, breast cancer, colon cancer, cirrhosis, sarcoidosis, and other autoimmune disorders.
Conditions associated with a monoclonal increase in the gamma region are as follows:
Smoldering myeloma
Monoclonal gammopathy of undetermined significance (MGUS)
Polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy, and skin changes (POEMS syndrome)
Solitary plasmacytoma
Castleman disease
AL amyloidosis
Heavy chain deposition disease
Light chain deposition disease
Polyclonal gammopathy
Infectious, Inflammatory or various reactive processes may be associated with a broad-based peak or band in the gamma region (Figure 4). This pattern suggests a polyclonal increase in immunoglobulins. Liver disease, autoimmune disease, chronic viral or bacterial infections and various malignancies may cause a polyclonal rise in the gamma fraction (see Table 2 below).
Considerations
The presence of an M-protein may be missed if the level is too small to be detected using SPEP. In cases where a high suspicion for a clonal plasma cell disorder is high, more sensitive tests such as a serum immunofixation or free light chain assay should be performed. In addition, when either alpha-1 antitrypsin deficiency or immunoglobulin deficiency, specific quantitation is indicated as SPEP is insensitive in these cases.
Background
Description
Serum protein electrophoresis (SPEP) is an easy, inexpensive method of separating proteins based on their net charge, size, and shape. The 2 major types of protein present in the serum are albumin and the globulin proteins. Albumin is the major protein component of serum and represents the largest peak that lies closest to the positive electrode. [1] Globulins make up a much smaller fraction of the total serum protein but represent the primary focus of interpretation of serum protein electrophoresis. Five globulin categories are represented: alpha-1, alpha-2, beta-1, beta-2, and gamma, with the gamma fraction being closest to the negative electrode (see the image below).
Indications/Applications
Serum protein electrophoresis is generally considered in any patient with an elevated total protein, especially those with elevated globulin level relative to albumin, or any signs and symptoms suggestive of an underlying plasma cell disorder such as multiple myeloma, Waldenstrom’s macroglobulinemia, or primary amyloidosis. [5] These include any of the following:
Unexplained anemia, back pain, bone pain, fatigue
Unexplained pathologic fracture or lytic lesions
Unexplained peripheral neuropathy
Hypercalcemia secondary to possible malignancy
Hypergammaglobulinemia
Rouleaux formation noted on peripheral blood smear
Renal insufficiency with bland urine sediment
Unexplained proteinuria
Bence Jones proteinuria [10]
Recurrent infections