Note to myself: This episode was good but I don’t need to review it or the notes again. The graphics from the show notes cover all the points that I want to remember for #236 Physical Exam Series: Approach to Shortness of Breath, OCTOBER 12, 2020 By DR JUSTIN BERK.
So I’m going through my past posts on the subject in my post, Dyspnea And Shortness Of Breath: A Review Of My Past Posts
Posted on November 5, 2020 by Tom Wade MD
But for now, here are excerpts from #236 Physical Exam Series: Approach to Shortness of Breath:
Summary
Learn which exam maneuvers are worthwhile and which ones are worthless in your approach to shortness of breath. In our evidence based series on the physical exam, we discuss the approach to the dyspneic patient with Dr. Brian Garibaldi (Hopkins, SBM), associate professor of pulmonary and critical care medicine at Johns Hopkins, and co-president of the Society of Bedside Medicine. We discuss the physical exam’s effect on our differential diagnosis, maneuvers that are commonly taught, and some simple tests with great data that may go overlooked. Be prepared, this episode may take your breath away!
Physical Exam Series: Approach to Shortness of Breath Clinical Pearls
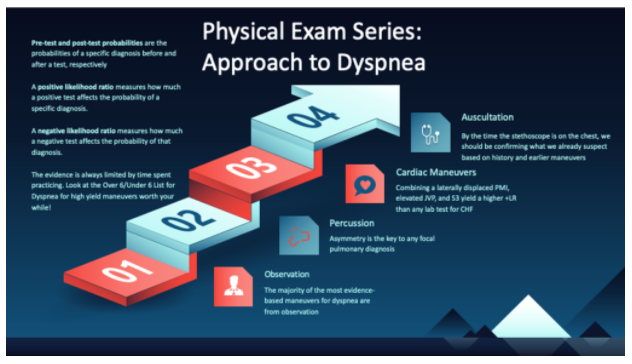
- By the time we put the stethoscope on the chest, we should be confirming what we already suspect based on prior exam maneuvers, history, and observation.
- Time is a diagnostic tool. It can be used to adjust the pre-test probability
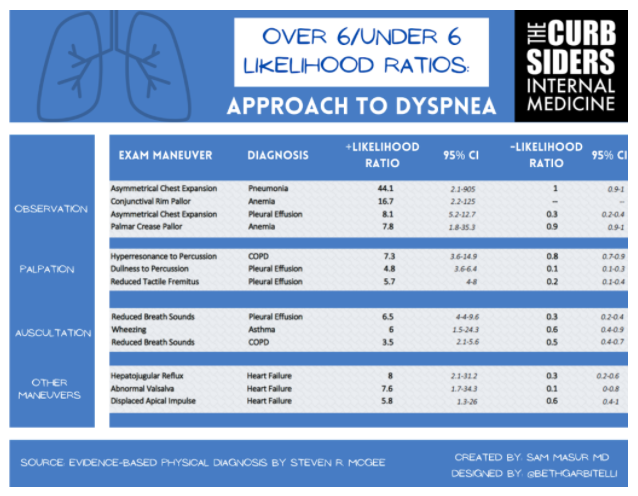
- Most maneuvers on the Over 6/Under 6 List for Dyspnea are not auscultation
- It is important to look at both the positive and negative likelihood ratios. For many tests, such as displaced PMI, they can be useful if positive, but their absence does not rule out the diagnosis.
- Practice. Dr. Garibaldi recommends being intentional with practice, including performing the maneuver on patients with and without positive findings.
- Dr. Garibaldi recommends asking others for their thoughts. Ask colleagues to come perform their exam maneuvers and compare notes.
- If interested in a certain part of the body, we must look at it completely. For example, don’t drop the stethoscope down someone’s shirt, hoping it will land on the heart.
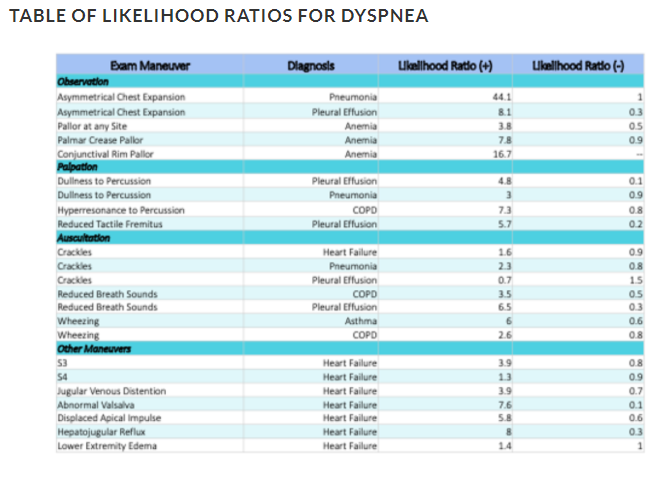
Likelihood Ratios*:
*For a more complete explanation than below, pleases see Diagnostics and Likelihood Ratios, Explained [It is brief but understandable] from The NNT – Quick summaries of evidence-based medicine.
- Each exam maneuver is a clinical test, with its own characteristics, such as sensitivity and specificity for a given diagnosis.
- Using these characteristics, we can calculate a likelihood ratio, which can be used to adjust our post-test probability for that diagnosis.
- A positive likelihood ratio measures how much a positive test affects the probability of a specific diagnosis.
- A negative likelihood ratio measures how much a negative test affects the probability of that diagnosis.
- Using Fagan’s Nomogram for likelihood ratios
- LR > 10 will change post test probability by 50% or more
- LR > 5 will change post test probability by 40%