“Low And Slow” refers to the hypotension and bradycardia that can occur with calcium channel and beta blocker overdose.
Today I’m reviewing calcium channel blocker overdose and beta blocker overdose. The two resources below are out standing podcast. The first is from the MCDC Paramedic Podcast and the second is from Emergency Medicine Cases.
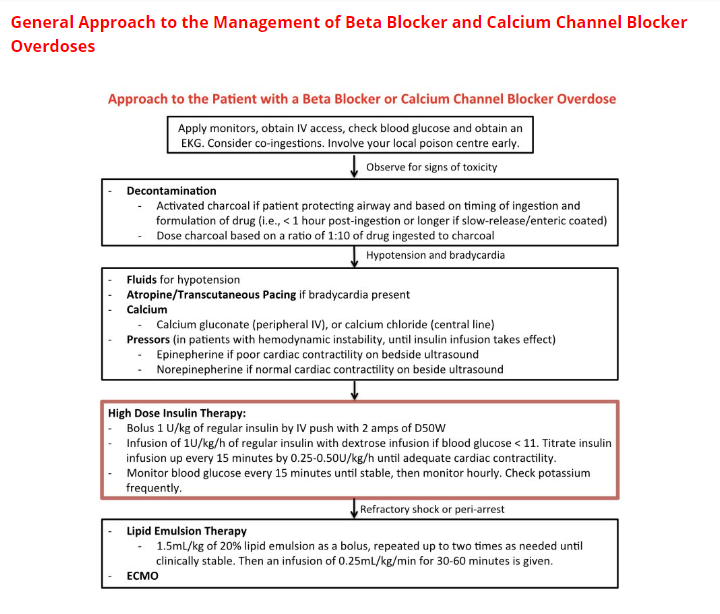
Here is the link to Episode 36 – Calcium Channel Blocker And Beta Blocker Toxicity from the MCDC Paramedic Podcast. And here are the show notes:
Cardiovascular medication poisoning can produce markedly unstable patient presentations. Dr. Patrick and Brad Ward review some of the basics and more recent therapeutic developments in the treatment and management of beta-blocker and calcium channel blocker toxicity.
References:
1. St-Onge M, Anseeuw K, Cantrell FL, et al. Experts Consensus Recommendations for the Management of Calcium Channel Blocker Poisoning in Adults. Critical Care Medicine. 2017;45(3):e306-e315.
2. Wax P, Erdman A, Chyka P, et al. Beta-blocker ingestion: an evidence-based consensus guideline for out-of-hospital management. Clin Toxicol (Phila). 2005; 43(3):131-146.
Here is the link to Episode 90 – Low and Slow Poisoning from Emergency Medicine Cases. And here are excerpts from the excellent show notes:
One of the things we need to think about whenever we see a patient who’s going low and slow with hypotension and bradycardia is an overdose. B-blockers, calcium channel blockers (CCB) and digoxin are some of the most frequently prescribed cardiovascular drugs. And inevitably we’re going to be faced with both intentional and unintentional overdoses from these drugs in the ED. On this EM Cases podcast the Medical Director of The Ontario Poison Control Centre and Emergency Physician at St. Michael’s Hospital, Dr. Margaret Thompson, along with Dr. Emily Austin, Emergency Physician and Toxicologist at St. Michael’s Hospital, help us to recognize these overdoses early and manage them appropriately.
Differential Diagnosis of Low and Slow
Non-toxicological causes:
- MI with cardiogenic shock
- Hyperkalemia
- Myxedema coma
- Spinal cord injury
- Hypothermia
Toxicological causes:
- Calcium channel blockers
- Beta-blockers
- Digoxin
- Opiates
- Alpha-2 antagonists (e.g., clonidine)
- Sodium channel blockers (e.g., TCA, carbamazepine, flexeril, antipsychotics, propranolol, cocaine)
Management of Seizures in the Toxicology Patient
There are several modifications of the usual algorithm for treating adult seizures when it comes to the poisoned patient.
Avoid Sodium Channel Blockers
Benzodiazepines are the first line treatment for treating seizures in patients with an overdose. In toxicological seizures, do not treat with antiepileptic drugs that have sodium channel blockade (i.e., phenytoin, fosphenytoin) because many poisons block sodium channels and additional sodium channel blockade may result in cardiac instability. If seizures persist, even after large doses of benzodiazepines, consider advancing to phenobarbital or propofol.
Bicarbonate
In patients with an overdose who are seizing and have evidence of sodium channel blockade (wide QRS on EKG), give sodium bicarbonate.
Naloxone
Consider naloxone in patients who may have an opioid overdose and are seizing. Some opioids can cause seizures (i.e., meperidine). Opioids may also cause hypoperfusion, which can lead to seizures.