
The following is from Resource (1) below:
Multiple myeloma (MM) is characterized by the neoplastic proliferation of plasma cell clones that produce monoclonal immunoglobulin. These plasma cell clones proliferate in the bone marrow causing skeletal damage, a hallmark of MM. Other disease related complications include hypercalcemia, renal insufficiency, anemia, and infections. MM accounts
for approximately 1.8% of all cancers and slightly more than 17% of hematologic malignancies in the United States. The American Cancer Society has estimated that 30,280 new MM cases will occur in the United States in 2017, with an estimated 12,590deaths. [Resource (1) below]
The following is from Resources (2) and (3) below:
Multiple myeloma (MM) [Link is to Resource (2) below] is a debilitating malignancy that is part of a spectrum of diseases ranging from monoclonal gammopathy of unknown significance (MGUS) [Link is to Resource (3) below]) to plasma cell leukemia.
Solitary plasmacytoma (SP) [Link is to Resource (4) below] is an early-stage plasma cell malignancy that is in between monoclonal gammopathy of undetermined significance (MGUS) and multiple myeloma (MM) along the spectrum of plasma cell disorders. [1] . A plasmacytoma is a discrete, solitary mass of neoplastic monoclonal plasma cells. SPs can be divided into 2 groups according to location:
Solitary bone plasmacytoma (SBP) – These occur most commonly in the vertebrae
Extramedullary plasmacytoma (EMP) – These encompass all nonosseus SPs; they can occur in any soft tissue but the upper airway tract, including the sinuses, is the most common site.
The following is from Resource (3) below:
MGUS represents two thirds of all plasma cell dyscrasias. The incidence increases with age. MGUS occurs in up to 5.3% of the population older than 70 years. [11]
The annual risk of progression [of MGUS] to multiple myeloma (MM), Waldenström macroglobulinemia (WM), amyloidosis (AL), or other lymphoproliferative disorders is 1% with IgG or IgA MGUS. This risk is 1.5% with IgM MGUS. A high plasma cell labeling index suggests active disease. Circulating plasma cells are an adverse predictor of progression.
The following is from Resource (4) below:
The rest of what follows are all excerpts from Resource (2) below.
First described in 1848, Multiple Myeloma (MM) is characterized by a proliferation of malignant plasma cells and a subsequent overabundance of monoclonal paraprotein (M protein).
MM is characterized by neoplastic proliferation of plasma cells involving more than 10% of the bone marrow.
MM can range from asymptomatic to severely symptomatic with complications requiring emergent treatment. Presenting signs and symptoms of MM include the following:
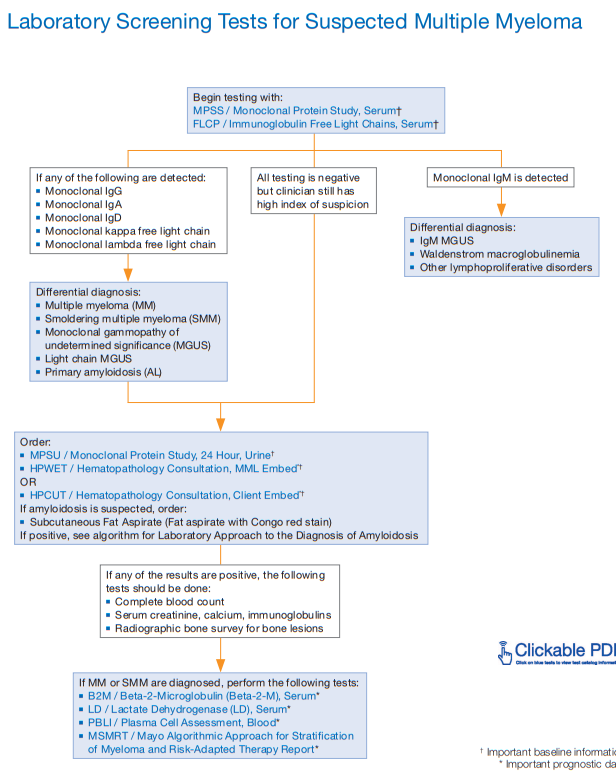
The International Myeloma Workshop guidelines for standard investigative workup in patients with suspected MM include the following [Resource (7) below. See also Resource (4) [Also the chart above] below on screening tests for multiple myeloma from Mayo Clinic Laboratories]
Imaging studies
Resources:
(1) NCCN Guidelines® Insights Multiple Myeloma, Version 3.2018
Featured Updates to the NCCN Guidelines [Abstract] [Full Text HTML] [Full Text PDF].
(2) Multiple Myeloma Updated Jan 11, 2018 from Emedecine.Medscape.com
(3) Monoclonal Gammopathies of Undetermined Significance Updated: Jul 06, 2017 from Emedecine.Medscape.com
(4) Solitary Plasmacytoma Updated: May 15, 2018 from Emedecine.Medscape.com.
(5) Laboratory Screening Tests For Multiple Myeloma [the link is to an awesome clickable PDF – you can click on every test in the flow chart and be taken to more information on that test] from Mayo Clinic Medical Laboratories.
(6) Multiple myeloma: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Ann Oncol. 2017 Jul 1;28(suppl_4):iv52-iv61. doi: 10.1093/annonc/mdx096.
(7) Consensus recommendations for standard investigative workup: report of the International Myeloma Workshop Consensus Panel 3 [Medline Abstract] [Full Text HTML] [Full Text PDF]. Blood. 2011 May 5;117(18):4701-5. doi: 10.1182/blood-2010-10-299529. Epub 2011 Feb 3.



