
CRACKCast, from CanadiEM, is a podcast that summarizes Rosen’s Emergency Medicine, chapter by chapter. I just listened to my first podcast, Chapter 4-Procedural Sedation and Analgesia [link is to the podcast and show notes page]-it is an excellent review. So this post is simply my reminder to me of how to access this resource.
A great compliment to the podcast above is Clinical Policy: Procedural Sedation and Analgesia in the Emergency Department 2014 [Link is to PDF Download] From the American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee).
For me the best way to follow along the podcast with the PDF show notes (they are outstanding).
Here are a few of the things to be remembered from the podcast and show notes:
recovery and discharge:
• must be back to baseline
• should not drive for 12-24 hrs
• should be supervised for at least 4-8 hrs post procedure**simple rule of thumb: don’t leave the bedside until the patient is able to vocalise**
7. List 8 complications / side effects of Ketamine + and how can the first four be managed?
1. hypersalivation / increased secretions
2. emesis3. laryngospasm
a. treatment not addressed in Rosen’s:
i. PPV with BVMpeep
ii. Jaw thrust
iii. Paralysis and intubation
See my post Ketamine Induced Laryngospasm for more information and resources on its management.
4. emergence reactions
a. only give pre-ketamine benzo’s for mitigating pre- procedural anxiety, not for everyone prophylactically; treat if you have a pt. with post-ketamine emergence reaction
b. giving ketamine at a slow rate helps limit the transient apnea, laryngospasm, and emesis/nausea
5. transient apnea (if given quickly)
6. ? increased IOP
7. worsening psychosis (hallucinogenic effects)
8. catecholamine surge phenomenon
9. Historic thought that it increased ICP8. List 4 situations when ketamine may be contraindicated?
laryngospasm concerns1. infants < 3 months
2. children with ongoing URTIs
Relative Contraindications to ketamine
3. Psychosis (acute or even well controlled!)
4. globe rupture (increasing IOP)
5. significant CAD (catecholamine surge..)
The above are just some of the great points in the podcast-shownotes.
One topic not mentioned in the podcast is being prepared for unexpected hypotension in procedural sedation with an already prepared syringe of push dose pressor.
[If you thought there was a real possibility of hypotension from even a semi-elective procedural sedation, you wouldn’t be doing it. You’d probably want to seek a consultation or additional hands on deck. So that’s why you want the syringe to be ready.]
The podcast also reminds us that most cases of hypoventilation from sedation can be managed with bag-valve mask ventilation.
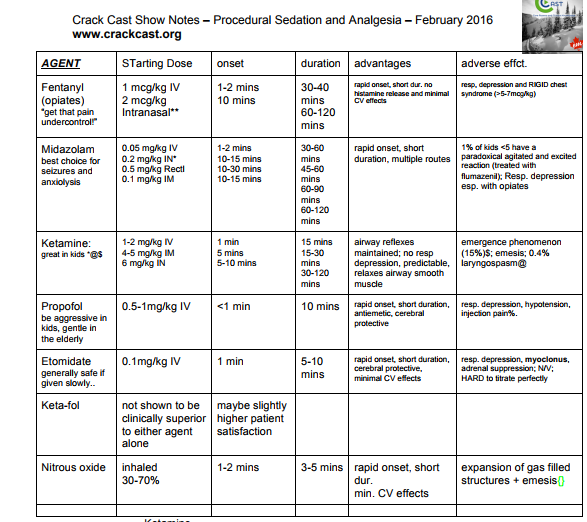
Here are two charts from the PDF:
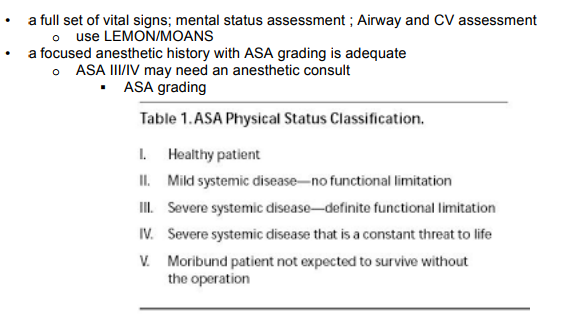
also from the above PDF:
Additional Resources:
(1) Clinical Policy: Procedural Sedation and Analgesia in the Emergency Department 2014 [Link is to PDF Download] From the American College of Emergency Physicians Clinical Policies Subcommittee (Writing Committee) on Procedural Sedation and Analgesia. Annals of Emergency Medicine, 63 (2014) 247-276. doi:10.1016/j



