The following are two articles on the technique of coronary CT angiography.
- Abbara S, Blanke P, Maroules CD, Cheezum M, Choi AD, Han BK, Marwan M, Naoum C, Norgaard BL, Rubinshtein R, et al. SCCT guidelines for the performance and acquisition of coronary computed tomographic angiography: a report of the society of Cardiovascular Computed Tomography Guidelines Committee: Endorsed by the North American Society for Cardiovascular Imaging (NASCI). J Cardiovasc Comput Tomogr. 2016;10:435–449.
2. Shaw LJ, Blankstein R, Bax JJ, Ferencik M, Bittencourt MS, Min JK, Berman DS, Leipsic J, Villines TC, Dey D, et al. Society of Cardiovascular Computed Tomography/North American Society of Cardiovascular Imaging—expert consensus document on coronary CT imaging of atherosclerotic plaque. J Cardiovasc Comput Tomogr. 2021;15:93–109.
PubMed Abstract There are 101 similar articles in PubMed The above article has been cited by 99 articles in PubMed
In today’s post, I review, and excerpt from reference 2: Society of Cardiovascular Computed Tomography/North American Society of Cardiovascular Imaging—expert consensus document on coronary CT imaging of atherosclerotic plaque. J Cardiovasc Comput Tomogr. 2021;15:93–109. Link is to the PDF.
All that follows is from the above resource.
Abstract
Coronary computed tomographic angiography (CCTA) provides a wealth of clinically meaningful information beyond anatomic stenosis alone, including the presence or absence of nonobstructive atherosclerosis and high-risk plaque features as precursors for incident coronary events. There is, however, no
uniform agreement on how to identify and quantify these features or their use in evidence-based clinical
decision-making. This statement from the Society of Cardiovascular Computed Tomography and North
American Society of Cardiovascular Imaging addresses this gap and provides a comprehensive review of
the available evidence on imaging of coronary atherosclerosis. In this statement, we provide standardized definitions for high-risk plaque (HRP) features and distill the evidence on the effectiveness of risk stratification into usable practice points. This statement outlines how this information should be communicated to referring physicians and patients by identifying critical elements to include in a structured CCTA report – the presence and severity of atherosclerotic plaque (descriptive statements, CAD-RADS™ categories), the segment involvement score, HRP features (e.g., low attenuation plaque, positive remodeling), and the coronary artery calcium score (when performed). Rigorous documentation of atherosclerosis on CCTA provides a vital opportunity to make recommendations for preventive care and to initiate and guide an effective care strategy for at-risk patients.
© 2020 Published by Elsevier Inc. on behalf of Society of Cardiovascular Computed Tomography.The traditional approach to imaging of coronary anatomy with
coronary computed tomographic angiography (CCTA) has been
oriented toward the detection of obstructive coronary artery disease (CAD). Over the past decade, evidence has accumulated concerning the prognostic significance of nonobstructive and
obstructive atherosclerotic plaque including specific features that are associated with an elevated risk of major adverse CAD events (MACE). This evidence now supports that imaging of atherosclerotic plaque is important for estimating patient risk and guiding preventive care. This link between initiation and intensification of prevention with atherosclerotic imaging using CCTA is vital to improving patient outcome. In this statement from the Society of Cardiovascular CT (SCCT) and North American Society of Cardiovascular Imaging (NASCI), we provide a synthesis of evidence concerning CCTA imaging of atherosclerosis and propose data elements that radiologists and cardiologists can integrate into their CCTA interpretation. One vital part of this statement is to acknowledge the advantages and limitations of current methods used to assess atherosclerotic plaque and to identify future research in this area. In this SCCT/NASCI statement, we enlist thought leaders in the field of CCTA including experts from the field of radiology and cardiology who bring unparalleled experience to this subject of atherosclerotic imaging. This field is rapidly evolving and
further advancements, including fully automated quantification of atherosclerotic plaque will necessitate future updates to this
statement.This statement focuses on the following principal issues that will influence how we think about imaging coronary atherosclerotic plaque:
1. CT Imaging of Atherosclerotic Plaque: Risk prediction in stable and unstable chest pain syndromes
2. Evidence Gaps in Coronary Atherosclerotic Plaque Imaging and Future Research Needs
3. CT Plaque Imaging to Direct Risk-Reducing Preventive or Disease-Modifying Therapies: Observational evidence on CCTA guided preventive strategies
4. Minimum Data Elements for Structured Reporting For Coronary Atherosclerotic Plaque
5. Consensus Summary and Recommendations1. Coronary atherosclerosis is the primary disease process
Imaging has traditionally focused on detecting flow limiting
stenosis or its surrogates. Detection of the presence and severity of
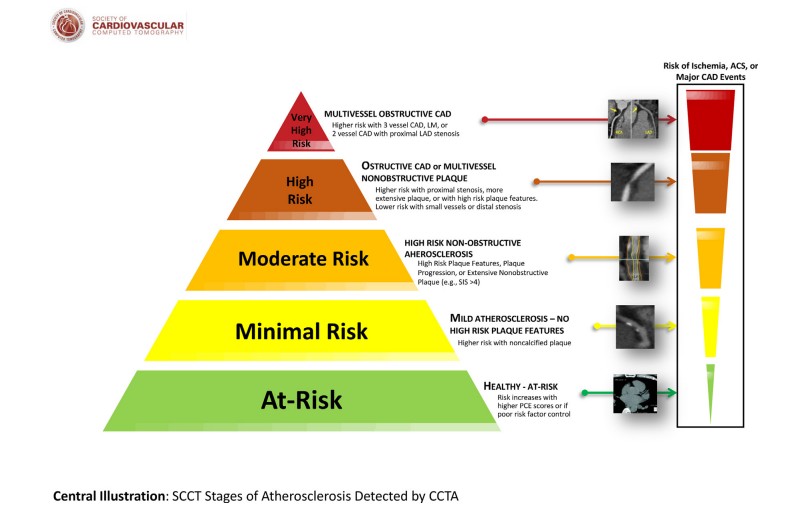
obstructive CAD by CCTA guide clinical decision making for secondary prevention including consideration of coronary revascularization. However, atherosclerosis is the primary disease process that mediates risk and stenosis is just one of its many subsets. Importantly, for risk assessment, patients with more extensive, multivessel CAD are at highest risk while those without any plaqueor stenosis comprise those at lowest risk (Central Illustration).
This document focuses on the presence and extent of atherosclerotic plaque that elevates risk above that of patients
without any documented plaque. This ranking of disease presence and severity remains vital to providing a comprehensive assessment of patient risk.The evolving paradigm for CCTA imaging represented in this
document expands this viewpoint beyond detecting obstructive
lesions to imaging coronary vessel pathology itself: characterizing and providing measurement of the burden of atherosclerosis, identifying how its composition influences risk and outcomes, and potentially modifying risk with initiation or intensification of therapy. We propose that imaging of atherosclerotic plaque in order to target effective preventive care strategies reinforces the concept that early detection and intervention has the greatest potential for improved event-free life years for at-risk patients. However, current randomized trials are lacking and do not proscribe a detailed evaluation and treatment pathway. In this statement, we synthesize the observational evidence and patterns as they unfold about
the impact of treatment on atherosclerotic plaque.