
Here is the home page of The Clinical Problem Solvers.
Here is The Clinical Problem Solvers’ page listing of Diagnostic Schemas for liver disease
Here is the link to the home page for Virtual Morning Report [From this link you can directly access all 572 episodes].
Virtual Morning Report–Episode 569 – Virtual Morning Report – January 26 – Acute liver injury [Watch on the Clinical Problem Solvers What follows is from the above resource.]
Case presenter – Ann Marie
Case overview & teaching points – Here
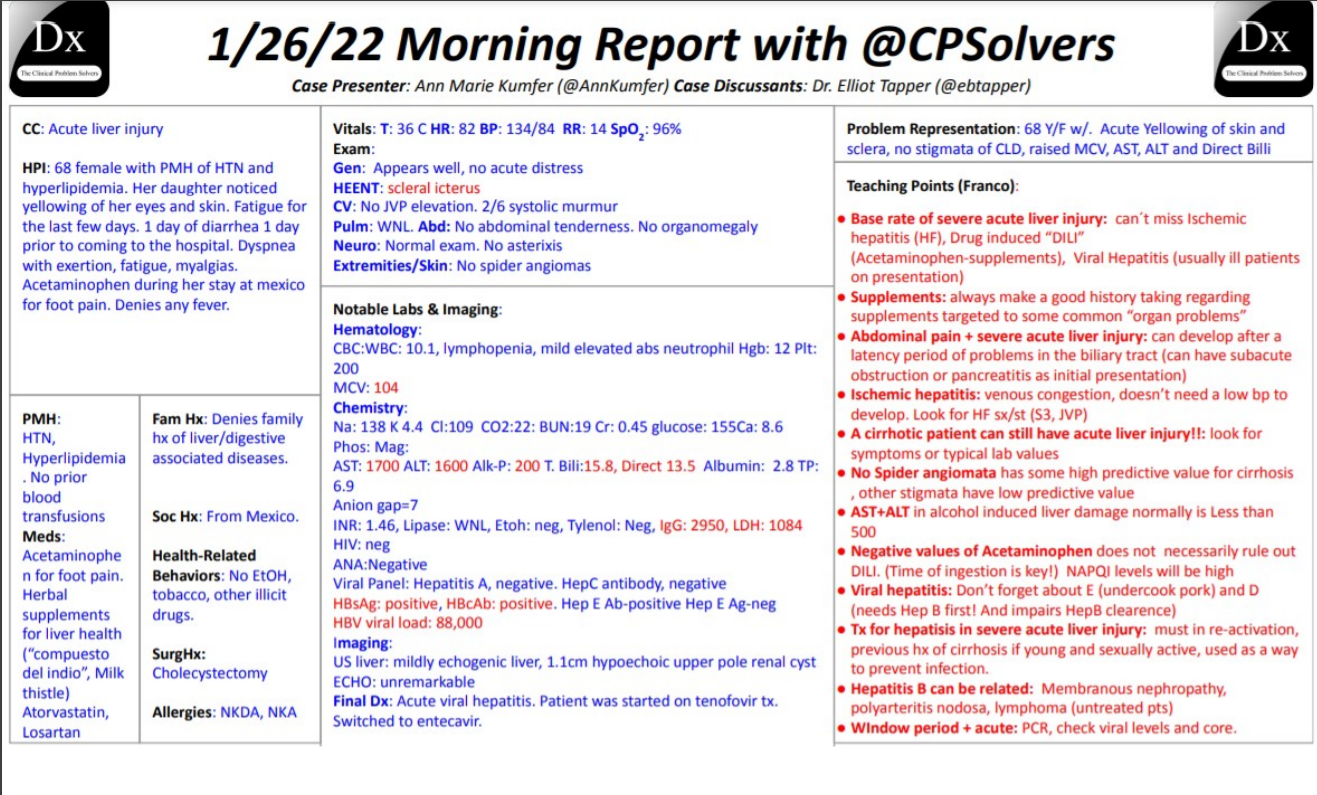
Note that Dr. Tapper states that the most common cause of acute liver injury is ischemic hepatitis from heart failure. Dr. Farkas in an IBCC chapter states that there need not be hypotension in this disease. [Personal thought: If ischemic hepatitis from heart failure is a common cause of acute liver injury, perhaps a VExUS exam should be included in the evaluation]

In this post I link to and excerpt from The YouTube Clinical Problem Solvers‘ “January 26, 2022 Hepatology VMR with Dr. Elliot Tapper – acute liver failure” [Link is to the video on YouTube]
By watching the video on YouTube, you can follow along in the autogenerated transcript which is usually adequate.
What follows is from the autogenerated transcript.
01:58one thing that i sometimes struggle with02:00an internist is the overlap between02:03alcohol use disorder and liver disease02:05do you have any pearls about if you have02:07concerned that someone may be developing02:09cirrhosis but it’s also02:12there is significant alcohol use that02:14could also be contributing to the02:15thrombocytopenia is there any way to02:17differentiate that02:20so you ask a very good question02:23and at the point that a patient is02:25developing some degree of bone marrow02:27suppression from alcohol use disorder02:29they’re already at an increased risk of02:32harm and if it’s important if that02:35patient needs extra reasons to be02:38worried about their health or motivated02:40about a change raising the possibility02:42of liver disease even when uncertain is02:45probably a useful tool and when you see02:48a patient like that i’m more than happy02:51to help sort things out either through02:54monitoring to see what happens after a02:56trial of substance use disorder therapy02:59doing non-invasive or liver biopsy03:02testing to figure out what’s going on03:03inside their liver and helping you03:06sort out exactly what your patient’s03:08stage might be03:12awesome well without further ado
03:26 [The internist is calling the hepatologist for]subspecialty care so the consult03:28question is going to be03:30severe acute liver injury03:33um so you’re going to be consulted about03:37lft rise with ast and alt in the03:41thousands as well as t-belly elevation03:45so just a little bit of background03:48story and then i’ll let you um ask kind03:52of some follow-up questions um and some03:54identifying details of this case have03:56been changed to protect identity03:59um so this is a 68 year old female with04:03a past medical history of hypertension04:05and hyperlipidemia04:07she is from mexico um but is visiting04:10her daughter um04:12in the east and um she04:16on presentation the daughter noticed04:18that um her eyes were yellow and she had04:20yellowing of the skin um she’s also been04:23very like04:24fatigued as well for the past 10 days um04:29they had not seen each other for the04:31past two weeks kind of other relevance04:34situations where there was and one day04:37of diarrhea04:39about a week prior to coming to the04:41hospital and then also some shortness of04:44breath with walking that was difficult04:46to quantify and have some diffuse04:49myalgias04:51but no04:52fevers or chills04:55she says she has been taking04:56acetaminophen um for04:59her chronic foot pain while in mexico um05:03but was unsure exactly how much she was05:05taking um05:07and then no recent travel05:11or nonstick contacts05:13no significant05:14alcohol use05:16um so at this point i know that you05:18don’t have all the exact laboratory data05:20but just kind of hearing this background05:22are there any specific05:24um questions or further evaluation have05:27you heard this consult question on the05:29phone that you would want to know about05:31right away
05:34um so i would say the i the first thing05:37that has set the way that i think about05:40this is i’ve been told this person has05:42severe acute liver injury and they have05:44jaundice and then you’ve gone on to05:46elaborate on a variety of other symptoms05:49that speak to a systemic process that05:52feels like it’s raising the possibility05:55of an infection or a toxic insult but05:59from behind the veil of ignorance just06:01going based on06:03epidemiology06:05alone there are really a very06:08limited number of things that can cause06:11a severe acute liver injury number one06:15will always be no matter which practice06:18setting you’re working in ischemic06:20hepatitis which typically happens in the06:23context of heart failure and i would06:26like to know you know what she what what06:29she looks like does she have cool clammy06:33extremities06:34then number two is going to be drug06:37induced liver injury you’ve piqued my06:40interest hearing about acetaminophen but06:43i want to know what else she is taking06:46and i’m looking for other sources of06:48acetaminophen i’ll oftentimes you’ll06:51hear people when they’re feeling bad06:52take both tylenol nyquil percocet all06:56things that would have acetaminophen in06:59them but i want to know the whole list07:01including the random supplements they07:04might be taking and i don’t remember07:06what which ones cause liver injury other07:09than like the common ones like07:11anti-epileptics and antibiotics so as07:13soon as you tell me that whole list i’m07:15plugging them into hepatology google07:18which is livertox.gov07:20and i’m looking to see what the rate of07:22liver injury on each of those might be07:24and then finally like i said07:26i worry about an infectious process the07:29third most common probability07:31possibility first for someone with this07:34kind of history07:35would be something like viral hepatitis07:38hepatitis a07:39potentially even07:41hepatitis
07:43b and rarely you will also see acute07:46hepatitis c so i’d want to know a little07:48bit about about the exposures to that07:51but i will definitely be testing for07:53those things no matter what the history07:56tells me
08:00awesome um just to give a little bit08:02more history and the patient had been



