
The following are excerpts from Reference 1, STOP-Bang Questionnaire: A Practical Approach to Screen for Obstructive Sleep Apnea:
There exists a high prevalence of OSA in the general population, a great proportion of which remains undiagnosed. The snoring, tiredness, observed apnea, high BP, BMI, age, neck circumference, and male gender (STOP-Bang) questionnaire was specifically developed to meet the need for a reliable, concise, and easy-to-use screening tool. It consists of eight dichotomous (yes/no) items related to the clinical features of sleep apnea. The total score ranges from 0 to 8. Patients can be classified for OSA risk based on their respective scores. The sensitivity of STOP-Bang score ≥ 3 to detect moderate to severe OSA (apnea-hypopnea index [AHI] > 15) and severe OSA (AHI > 30) is 93% and 100%, respectively. Corresponding negative predictive values are 90% and 100%. As the STOP-Bang score increases from 0 to 2 up to 7 to 8, the probability of moderate to severe OSA increases from 18% to 60%, and the probability of severe OSA rises from 4% to 38%. Patients with a STOP-Bang score of 0 to 2 can be classified as low risk for moderate to severe OSA whereas those with a score of 5 to 8 can be classified as high risk for moderate to severe OSA. In patients whose STOP-Bang scores are in the midrange (3 or 4), further criteria are required for classification. For example, a STOP-Bang score of ≥ 2 plus a BMI > 35 kg/m2 would classify that patient as having a high risk for moderate to severe OSA. In this way, patients can be stratified for OSA risk according to their STOP-Bang scores.
The STOP-Bang questionnaire includes the four questions used in the STOP questionnaire plus four additional demographic queries,20 for a total of eight dichotomous (yes/no) questions related to the clinical features of sleep apnea (snoring, tiredness, observed apnea, high blood pressure, BMI, age, neck circumference and male gender). For each question, answering “yes” scores 1, a “no” response scores 0, and the total score ranges from 0 to 8. The components of STOP questionnaire were selected based on the factor analysis of 14 candidate questions designed to reflect snoring, daytime tiredness, observed breathing cessation, and high BP.20
The questionnaire can be completed quickly and easily (usually within 1-2 min), and overall response rates are typically high (90%-100%).20 The questionnaire has demonstrated a high sensitivity using a cutoff score of ≥ 3: 84% in detecting any sleep apnea (AHI > 5 events/h), 93% in detecting moderate to severe sleep apnea (AHI > 15 events/h), and 100% in detecting severe sleep apnea (AHI > 30 events/h).20Corresponding specificities were 56.4%, 43%, and 37%.20 If patients score 0 to 2 on the STOP-Bang questionnaire, they are considered to be at low risk of OSA, and the possibility of those patients having moderate to severe sleep apnea can be confidently ruled out.
Because of its ease of use, efficiency, and high sensitivity, the STOP-Bang questionnaire has been widely adopted and validated in various populations and among patients with assorted medical conditions.
Association Between STOP-Bang Scores and Predictive Probability of OSA
Although the high sensitivity of the STOP-Bang questionnaire makes it useful as an OSA screening tool, it is possible that the modest specificity (43% to detect moderate to severe sleep apnea) will yield a high false-positive rate.20 This, in turn, could result in unnecessary referral to sleep clinics for polysomnography, as well as increase the cost of care for surgical patients owing to additional perioperative monitoring.
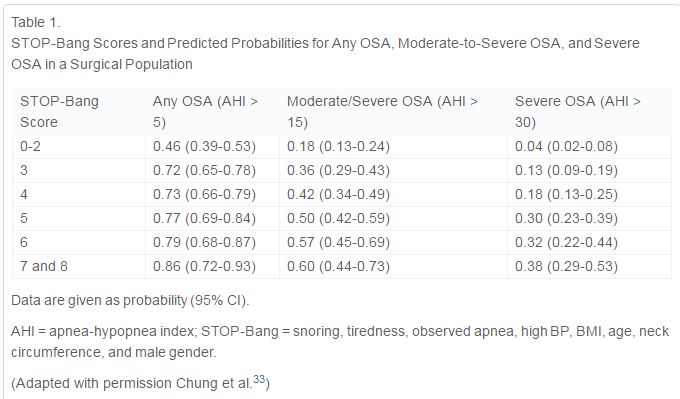
We discovered that as the STOP-Bang scores increased from 0 to 2 up to 7 to 8, the probability of moderate to severe OSA increased from 18% to 60% and the probability of severe OSA rose from 4% to 38% (Table 1).33
Alternative Models for Scoring the STOP-Bang Questionnaire
For ease of use, all items on the STOP-Bang questionnaire are treated equally for scoring purposes, using a count of 0 or 1. The items on the questionnaire do not share an equal predictive weight for OSA.14 and 20
[So we can weigh the scores differently to improve specifity – see below]
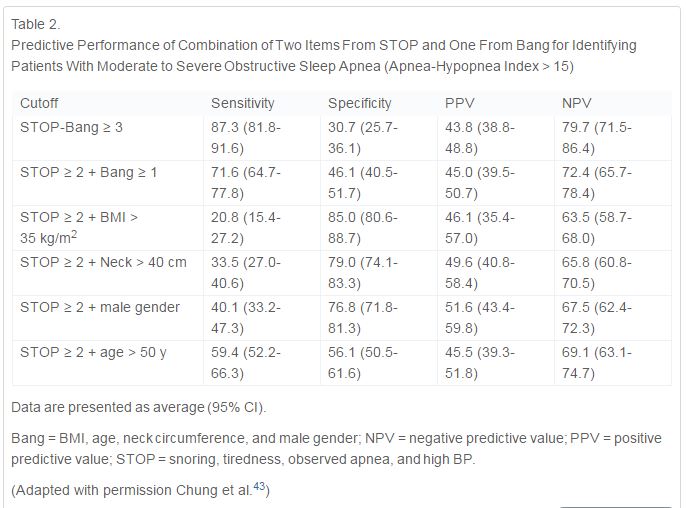
The predictive performance of specific combinations of items has also been explored.43 Compared with the specificity of 31% for detecting moderate to severe OSA using a combination of any three positive items on the STOP-Bang questionnaire, the following three combinations significantly improve the specificity to detect any OSA (AHI > 5), moderate to severe OSA (AHI > 15), and severe OSA (AHI > 30) at the expense of sensitivity: (1) STOP score ≥ 2 plus BMI > 35 kg/m2; (2) STOP score ≥ 2 plus neck circumference > 40 cm (16 in); and (3) STOP score ≥ 2 plus male gender.43 The specificity to detect moderate to severe OSA increases as follows based on those different combinations: to 85% for the combination of a STOP score ≥ 2 plus BMI > 35 kg/m2; to 79% for the combination of a STOP score ≥ 2 plus neck circumference > 40 cm (16 in); and to 77% for the combination of a STOP score ≥ 2 plus male. These valuable data can assist in accurately identifying more patients with moderate to severe OSA (Table 2).
The STOP-Bang Questionnaire and Serum Bicarbonate
Since nocturnal intermittent hypercapnia resulting from to obstructive apnea or hypopnea may lead to renal HCO3– retention to compensate for acute respiratory acidosis,47 it may subsequently result in elevated serum HCO3–. Our findings indicate that serum HCO3– is significantly correlated to AHI,48 and the addition of serum HCO3– ≥ 28 mmol/L to a STOP-Bang score ≥ 3 improves the specificity to predict moderate to severe OSA but decreases its sensitivity.48 Under that condition (a STOP-Bang score of ≥ 3 plus HCO3– ≥ 28 mmol/L), the specificity for detecting moderate to severe OSA increases from 30% to 82%, and from 28% to 80% for detecting severe OSA.48
Two-Step Strategy for Using STOP-Bang Questionnaire
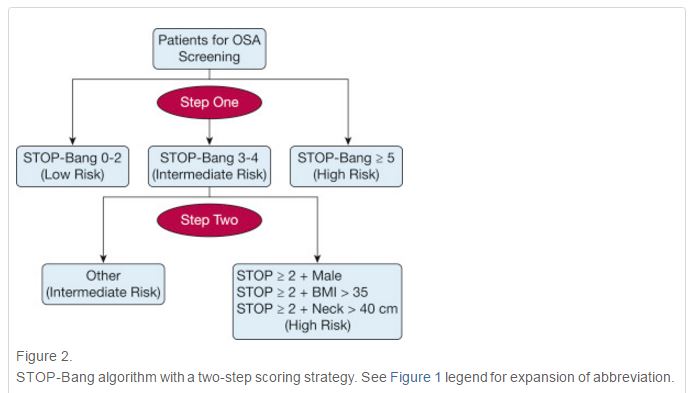
Based on these data,33, 43 and 48 we propose a two-step algorithm (Fig 2 ) to use the STOP-Bang questionnaire to identify patients effectively with a high probability of moderate to severe sleep apnea. As shown in Figure 2, the first step is to check the STOP-Bang score. If a patient scores 0 to 2 on the STOP-Bang questionnaire, he or she is unlikely to have moderate to severe OSA. Conversely, a patient with a STOP-Bang score of 5 to 8 has a high probability of having moderate to severe OSA (Table 1).33 The second step is for patients falling in the middle: those with STOP-Bang scores of 3 or 4. These patients can be further classified as having a higher risk for moderate to severe OSA if one of the following conditions is met: (1) the combination of a STOP score of ≥ 2 plus BMI > 35 kg/m2; (2) a STOP score of ≥ 2 plus male gender; (3) a STOP score of ≥ 2 plus neck circumference > 40 cm (16 in); or (4) a STOP-Bang score of ≥ 3 plus serum HCO3– ≥ 28 mmol/L. This two-step algorithm needs to be further validated prospectively.
STOP-Bang Questionnaire in the General Population and in Bus Drivers
Studies in primary care patients demonstrate that the STOP-Bang questionnaire has predictive performance similar to that seen in surgical and sleep clinic patients.34 and 35.
Resources:
The STOP-Bang Questionnaire [Full Text PDF] from the Federal Aviation Administration site.
STOP-Bang Questionnaire: A Practical Approach to Screen for Obstructive Sleep Apnea [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Chest. 2016 Mar;149(3):631-8. doi: 10.1378/chest.15-0903. Epub 2016 Jan 12.
Society of Anesthesia and Sleep Medicine Guidelines on Preoperative Screening and Assessment of Adult Patients With Obstructive Sleep Apnea [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Anesth Analg. 2016 Aug; 123(2): 452–473. Published online 2016 Jul 22. doi: 10.1213/ANE.0000000000001416



