
I’ve posted updated information on this subject, Links To And Excerpts From “Mildly Elevated Liver Transaminase Levels: Causes and Evaluation” From American Family Physician, posted on August 23, 2019 by Tom Wade MD.
So the post below is superseded. I’ve left it in for the above link.
This post contains links to and excerpts from from Resource (3) Causes and Evaluation of Mildly Elevated Liver Transaminase Levels [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Am Fam Physician. 2011 Nov 1;84(9):1003-8.
The reason we want to recognize ongoing liver damage as soon as possible is so that, hopefully, we can prescribe treatment to prevent damage from preceding from mild liver damage –> liver fibrosis –> cirrhosis –> portal hypertension –> the complications of liver failure +/or hepatocellular carcinoma.
It is important to thoroughly evaluate persistent mildly elevated AST and ALT because elevations can be a sign of ongoing liver damage that if untreated could go on to cirrhosis (and to the complications of chirrhosis: “ascites, spontaneous bacterial peritonitis, hepatic encephalopathy, portal hypertension, variceal bleeding, and hepatorenal syndrome [See References (1) and (2) for the diagnosis of cirrhosis and it’s complications]).
The figures and text that follows are all from reference (3) in resources:
Elevated liver enzymes (alanine transaminase [ALT] and aspartate transaminase [ALT]) are elevated in approximately 9% of people in the National Health and Nutrition Survey.
Most often these patients are asymptomatic and the elevated levels are mild (less than 5 times the upper limit of normal).
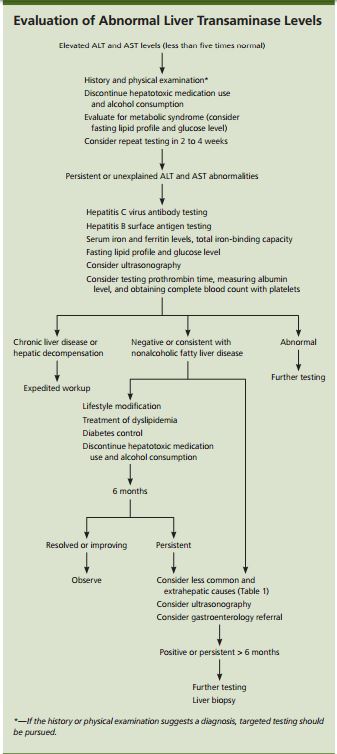
Understanding the basic disease processes that cause mildly elevated liver transaminase levels (i.e., less than five times the upper limit of normal) and the epidemiology of each disease can help guide the patient history, physical examination, and further diagnostic testing.
Etiologies
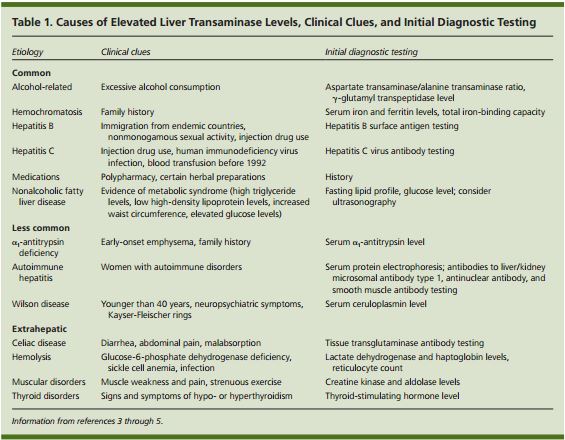
Hepatocellular damage releases ALT and AST into the bloodstream. ALT is found primarily in the liver; AST is also found in skeletal muscles and erythrocytes. Therefore, elevations in ALT levels generally are more specific for hepatic injury. At times, the AST/ALT ratio can suggest certain disease patterns. For instance, a ratio greater than 2 suggests alcoholic liver disease, whereas nonalcoholic fatty liver disease is usually associated with a ratio of less than 1. A ratio greater than 4 may suggest Wilson disease.6 When the AST/ALT ratio does not suggest an etiology, asymptomatic elevation of liver transaminase levels can be categorized into common hepatic, less common hepatic, and extrahepatic causes (Table 1).3–5
Common Causes
NONALCOHOLIC FATTY LIVER DISEASE [See also Reference (4) below]
Nonalcoholic fatty liver disease is the leading cause of mild transaminase elevations, and is becoming more prevalent as the obesity rate increases. It is estimated that 30 percent of U.S. adults have nonalcoholic fatty liver disease, and that up to 3 to 6 percent have nonalcoholic steatohepatitis.7 [And it is steatohepatitis can lead to cirrhosis and it’s complications.]
Nonalcoholic fatty liver disease is the leading cause of mild transaminase elevations, and is becoming more prevalent as the obesity rate increases. It is estimated that 30 percent of U.S. adults have nonalcoholic fatty liver disease, and that up to 3 to 6 percent have nonalcoholic steatohepatitis.7 [And it is steatohepatitis can lead to cirrhosis and it’s complications.]
Nonalcoholic fatty liver disease should be considered in patients who are obese or who have diabetes mellitus, hypertriglyceridemia, or the metabolic syndrome.8
Ultrasonography, computed tomography, and magnetic resonance imaging have fair to excellent sensitivity and specificity for identifying hepatic steatosis7,9,10(Table 210). Ultrasonography is the most common test for nonalcoholic fatty liver disease because of its wide availability and low cost.5,11 Imaging may assist in the diagnosis of nonalcoholic fatty liver disease, but not in the differentiation of hepatic steatosis from nonalcoholic steatohepatitis. A definitive diagnosis of nonalcoholic steatohepatitis is made when liver biopsy demonstrates inflammation and evidence of fibrosis not typically seen in hepatic steatosis.7
ALCOHOL
In a study of 256 asymptomatic Swedish patients with mildly elevated liver transaminase levels, alcohol was found to be the cause in 10 percent.12 The most important way to make the diagnosis is through an accurate history. Biopsy alone cannot differentiate alcoholic liver disease from nonalcoholic fatty liver disease. An AST/ALT ratio greater than 2 supports a diagnosis of alcoholic liver disease, as does an elevated γ-glutamyl transpeptidase level in the setting of an AST/ALT ratio greater than 2.
MEDICATIONS
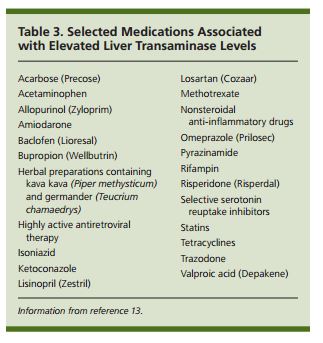
Numerous medications have been associated with elevated transaminase levels, but the true incidence of liver injury from medications is unknown. Eliciting all over-the-counter and prescription medications and stopping any potentially contributing agents may identify the etiology (Table 3).13 .
VIRAL HEPATITIS [See also Reference (3) below]
An estimated 3.2 million persons in the United States have chronic hepatitis C, and up to 1.2 million have hepatitis B.22,23 Hepatitis C can cause transient elevations in liver enzymes (typically ALT), and physicians should consider testing even if repeat liver enzyme testing is normal. Testing for hepatitis C virus antibody and hepatitis B surface antigen can identify patients with chronic hepatitis C and hepatitis B, respectively.
HEMOCHROMATOSIS [See Reference (4) below]
Hemochromatosis, a genetic disease of iron metabolism, can cause asymptomatic elevation of liver transaminase levels as a result of iron deposition in the liver. The gene mutation that causes hemochromatosis, C282Y, is relatively common among non-Hispanic whites. However, because of its variable penetrance, the prevalence is estimated to be only three to five per 1,000 persons who manifest the disease.24 Initial testing includes serum iron and ferritin levels, and total iron-binding capacity. Transferrin saturation greater than 50 to 55 percent and a serum ferritin level greater than 200 to 250 ng per mL (449.40 to 561.75 pmol per L) should prompt further testing for hemochromatosis.24
Less Common Causes
Α1ANTITRYPSIN DEFICIENCY [See also Reference (5) below]
α1Antitrypsin deficiency is a hereditary disease that causes chronic lung and liver disease. The prevalence is approximately one per 3,000 to 5,000 persons, but only 10 percent of those with the disease are clinically identified.25 This condition can cause varying degrees of liver disease, from asymptomatic elevation of transaminase levels to chronic liver disease, cirrhosis, and liver failure. The heterozygous form, which is found in 1.5 to 3 percent of the population, may worsen chronic liver disease from other causes.26 Measurement of serum α1antitrypsin is a reasonable first step in diagnosing this condition.3–5
AUTOIMMUNE HEPATITIS [See also Reference (6) below]
The prevalence of autoimmune hepatitis is 11 to 17 per 100,000 persons.27 It occurs more often in women and is commonly associated with other autoimmune disorders. Hypergammaglobulinemia is common, and the total gamma globulin or immunoglobulin G levels are generally 1.2 to 3.0 times normal.28 Serum protein electrophoresis testing has high sensitivity for autoimmune hepatitis, whereas antinuclear antibody testing has lower sensitivity and specificity.4 Other laboratory testing may include smooth muscle antibody and liver/kidney microsomal antibody type 1 testing.27
[This paragraph is from Autoimmune Hepatitis Workup from emedicine.medscape.com: Clinicians must consider the diagnosis of autoimmune hepatitis in any patient who has acute hepatitis or acute liver failure (defined by the new onset of coagulopathy). In addition to aminotransferase levels and other liver function studies, the workup of such patients should include the following assays:
- Serum antinuclear antibody (ANA)
- Anti–smooth muscle antibody (ASMA)
- Liver-kidney microsomal type 1 (LKM-1)
- antibody
- Serum protein electrophoresis (SPEP)
- Quantitative immunoglobulins]
Resuming Less Common Causes from Reference (1)
WILSON DISEASE [See also Reference (7)
Wilson disease is a rare autosomal recessive genetic disorder related to ineffective copper metabolism. It occurs in approximately one in 30,000 persons, is more common in Eastern Europeans, and generally presents before 40 years of age.29 Kayser-Fleischer rings (i.e., copper deposition around the cornea) and neuropsychiatric symptoms are key clinical clues. Serum ceruloplasmin measurement is typically the initial test.3–5 Low levels can be confirmed with genetic testing and liver biopsy.
Extrahepatic Causes
Several extrahepatic causes of asymptomatic elevations of liver transaminase levels can be pursued based on the clinical scenario. It is not clear how thyroid disorders elevate liver transaminase levels, but measurement of serum thyroid-stimulating hormone can help rule out this potential cause. Celiac disease has also been implicated in asymptomatic liver transaminase elevations; tissue transglutaminase antibody testing can have a role in this diagnosis.5 Hemolysis and strenuous exercise also may be potential causes. Muscle disorders such as rhabdomyolysis or polymyositis are unlikely in asymptomatic patients, but measurement of creatine kinase and aldolase may be reasonable in the appropriate clinical setting.
Resources:
(1) Cirrhosis and chronic liver failure: part I. Diagnosis and evaluation. [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Am Fam Physician. 2006 Sep 1;74(5):756-62.
(2) Cirrhosis and chronic liver failure: part II. Complications and treatment [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Am Fam Physician. 2006 Sep 1;74(5):767-76.
(3) Causes and Evaluation of Mildly Elevated Liver Transaminase Levels [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Am Fam Physician. 2011 Nov 1;84(9):1003-8.
(4) Nonalcoholic Fatty Liver Disease: Diagnosis and Management [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Am Fam Physician. 2013 Jul 1;88(1):35-42.
(5) Viral Hepatitis from emedicine.medscape.com
(6) Hereditary Hemochromatosis [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Am Fam Physician. 2013 Feb 1;87(3):183-90.
(7) Alpha1-Antitrypsin Deficiency from emedicine.medscape.com
(8) Autoimmune Hepatitis from emedicine.medscape.com
(9) Wilson Disease from emedicine.medscape.com
(10) EASL–EASD–EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease [PubMed Citation] [Full HTML] [Full Text PDF]. J Hepatol. 2016 Jun;64(6):1388-402. doi: 10.1016/j.jhep.2015.11.004. Epub 2016 Apr 7.
(11) The diagnosis and management of non-alcoholic fatty liver disease: Practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. [PubMed Citation] [Full Text PDF]. Hepatology. 2012 Jun;55(6):2005-23. doi: 10.1002/hep.25762.
(12) Cirrhosis from The National Institute of Diabetes and Digestive and Kidney Diseases
(13) Assessing Portal Hypertension In Liver Disease from www.medscape.org.
(14) Portal Hypertension Imaging from emedicine.medscape.com
(15) Hepatocellular Carcinoma from emedicine.medscape.com
(16) Acute Liver Failure from emedicine.medscape.com
(17) EASL-ALEH Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis [PubMed Citation] [Full Text HTML] [Full Text PDF]. J Hepatol. 2015 Jul;63(1):237-64. doi: 10.1016/j.jhep.2015.04.006. Epub 2015 Apr 21.
(18) Clinical Practice Guidelines from the Journal of Hepatology of The European Society for the Study of the Liver (EASL)
(19) Practice Guidelines from The American Association For The Study Of Liver Diseases
(20) Acute-on-chronic liver failure: A new syndrome that will re-classify cirrhosis [Pubmed] [Full Text HTML] [Full Text PDF]. J Hepatol. 2015 Apr;62(1 Suppl):S131-43. doi: 10.1016/j.jhep.2014.11.045.



