
Intranasal sedation for pediatric patients is a YouTube video (2013, 47:45) from pediatric emergency specialist Dr. Jay Pershad. What follows is from this video:
Start at 4:25 – first part is just introduction.
- Pharmacologic Principles
- PO vs Intranasal
- Bioavailability of PO meds is much lower and they take much longer to act than intransal.
- And if intransal med is administered correctly it is going to be absorbed directly into the systemic circulation
- Drug Volume/ Concentration
- You want to decrease drug volume as much as you can and you want to have the concentration of the medicine as high as possible.
- The concentration for midazolam, the medication that we prefer [for sedation], is 5 mg/cc, not 1 mg/cc.
- fentanyl, the medication we use for analgesia, comes as 50 micrograms/cc.
- Optimal Volume
- Optimal volume is .2 to .3 cc per nostril, with maximum of one cc per nostril.
- If you give more than one cc it is going to drip down and they will swallow it and defeat the purpose.
- Adequate Dosing
- The key point to remember is that it is higher than IV dosing.
- So if you’re using IV midazolam it might be giving 0.1 mg per kilo.
- But if you are giving intranasal midazolam, you may be giving 0.3 to 0.5 mg per kilo.
- The reason that the dose is higher than IV dose is because bioavailability, although better than po is still much less than IV dose.
- Utilizing both nostrils
- By utilizing both nostrils for your dose you increase the mucosal area available for absorption is maximized.
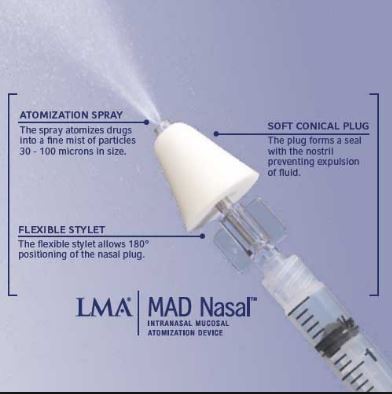
- Delivery (spray vs drops)
- Spray is better than drops because it is absorbed better than drops which will likely just run out from the front or back.
- And to spray you need an atomizer.
9:21
- Evidence Base
- A Randomized Clinical Trial Comparing Oral, Aersolized, Intranasal and Aerosolized Buccal Midazolam [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Ann Emerg Med. 2011 Oct;58(4):323-9. doi: 10.1016/j.annemergmed.2011.05.016.
- A Randomized Controlled Trial Comparing Intransal to Intravenous Morphine for Managing Acute Pain in the Emergency Department [PubMedAbstract]. Ann Emerg Med. 2007 Mar;49(3):335-40. Epub 2006 Oct 25.
16:05
- Practical Tips
- Inspect the nostrils for blood and mucous.
- Suction the nostrils for blood and mucous.
- If there is copious secretions than the intranasal route may not work.
- Forewarn! Midazolam will burn for about 30 seconds.
- “Dead space” in the atomizer. You have to factor that in your administration. So maybe you want to give just a touch extra. ‘”So you may want to go up by 0.1 or 0.2cc. You’ve to factor that into your administration.”
- Titration
- Monitoring?
- At the time of this video, Dr. Pershad says that we don’t monitor patient if they are only receiving midazolam. (Check your hospital policy.
- If we are using intranasal midazolam and intransal fentenyl together, we do put the patient on the monitors.
20:40
- Rang of Indications
- Laceration Repair
- Example: a 2 year old with a large forehead laceration.
- Our current options are:
- give IM ketamine because you can’t reason with a 2 year old.
- Just hold him down – that’s not acceptable, we can do better than that.
- So here we would give the patient intranasal midazolam and wait 15 minutes for it to kick in and then go ahead and inject the laceration.
- Or if you are using LAT Gel*, apply it at T minus 30 minutes, give the intranasal midazolam at T minus 15 minutes and then at time 0, we’re ready to suture.
*LAT gel is a topical anaesthetic gel that can be applied to open wounds. • LAT gel reduces the need to inject local anaesthetic/sedation when cleaning and suturing open wounds in paediatric patients. [Download LAT gel for paediatric wounds Guideline, 2004, Cambridge University Hospitals, NHS Foundation Trust]. See also LAT gel, a powerful tool underused in the repair of paediatric lacerations. [PubMed Abstract]. Int J Oral Maxillofac Surg. 2014 Aug;43(8):955-6. doi: 10.1016/j.ijom.2014.04.014. Epub 2014 May 24.
- Fractures
- I + D
- You can use intranasal midazolam along with a local anesthetic cream – EMLA cream.
- Bladder Catheterization
- Peripheral IV
- You can use intranasal midazolam to start an IV. Once you have an IV your options are enormous.
- CT Imaging
- Status Epilepticus
- You can give intranasal midazolam while you are supporting the airway before you even have an IV. [But remember that another alternative is to give IM midazolam .]
- Opiod Overdose
- While you are supporting the airway, you can give intranasal naloxone.
25:42 to 30:06
- Chart of the Meds With Dosages For Intranasal Administration and a discussion of the meds.
- Because the chart did not reproduce clearly on my screen I did not include it or his discussion.
- Instead, I suggest you visit intranasal.net*
*intranasal.net – Therapeutic Intranasal Drug Delivery: Needleless treatment options for medical problems. From the site:
Why you should consider intranasal drug administration as another option for delivering medications to patients:
Acute seizures, status epilepsy, heroin and narcotic overdose, insulin induced hypoglycemia, procedural sedation, and acute and chronic pain control are all complex medical problems requiring multiple approaches for effective management. Intranasal drug delivery is emerging as a low-tech, inexpensive and non-invasive first line method for managing selected patients with these and other medical problems. Nasal medication delivery takes a middle path between slow onset oral medications and invasive, highly skilled delivery of intravenous medications. Because the nasal mucosa is highly vascularized, delivery of a thin layer of medication across a broad surface area can result in rapid transmucosal absorption of the medication into the blood stream and cerebral spinal fluid. This results in therapeutic drug levels and effective treatment of seizures, pain, anxiety, hypoglycemia, opiate overdose, epistaxis (bloody noses), etc without the need to give a shot or a pill. Because intra-nasal medication delivery is effective using generic medications, it is quite inexpensive, an advantage in this era of increasingly expensive medical technology. This web site provides information in the form of medical research, expert testimonial opinion and protocol suggestions to health care providers and consumers regarding this emerging method of drug delivery.
From 30:06 to the End: Dr. Pershad answers questions.
Additional Resources:
How to give your child midazolam 4:00 YouTube video
Intranasal Medications In Pediatrics
Posted on July 12, 2016 by Tom Wade MD



