Today I once again reviewed Dr. Josh Farkas‘ outstanding Internet Book of Critical Care [link is to the Table Of Contents] chapter, Atrial Fibrillation (AF) & Flutter complicating critical illness, Jan 6, 2017.
Please also see and review the Internet Book Of Critical Care‘s [Link is to the Table Of Contents] chapter, Bradycardia, by Dr. Josh Farkas, January 2017.
All that follows is from the Atrial fibrillation chapter.
CONTENTS
- Rapid Reference
- Introduction
- Diagnosis of AF
- Prevention of AF
- Investigation of the cause of AF
- Management – Overall approach
- Atrial flutter
- Podcast
- Questions & discussion
- Pitfalls
rapid reference
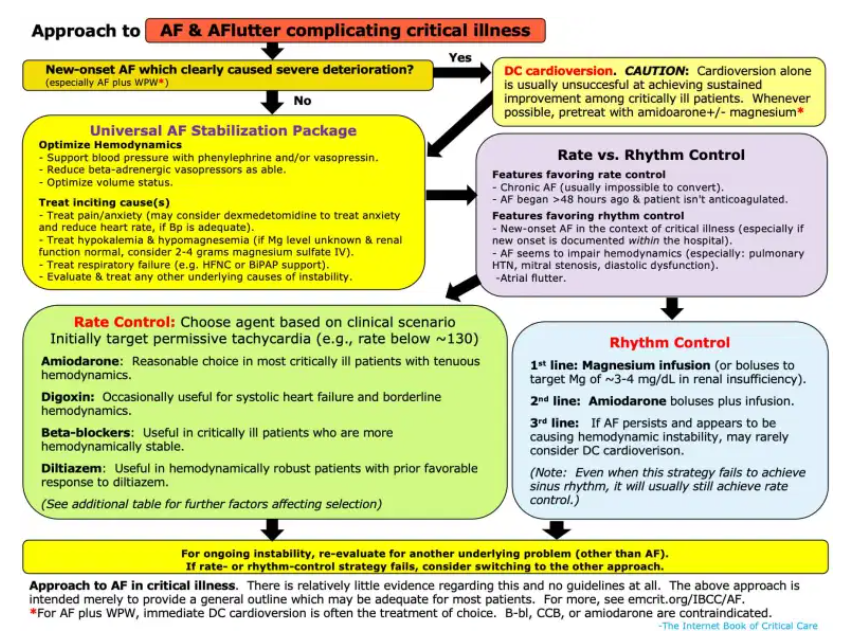
overall approach:
agent selection for rate control:
introduction
what this chapter is about
- AF is the most common arrhythmia encountered in the ICU.(29627355) The two most common scenarios are:
- (1) A patient with chronic AF develops critical illness.
- (2) A patient who was previously in sinus rhythm develops new-onset AF (NOAF) while in the ICU, secondary to the physiologic stress of critical illness (e.g., secondary to sepsis or pulmonary embolism).
- These situations are different from AF in other contexts, for example:
- ICU patients are often hemodynamically tenuous, so they may respond poorly to the usual AF therapies (e.g., diltiazem).
- DC cardioversion alone has a low success rate among critically ill patients (patients will usually revert back into AF).
- The optimal heart rate for critically ill patients is unknown, but some patients may benefit from a mild compensatory tachycardia. Immediately pushing the heart rate down to a “normal” range (e.g., <100) can be dangerous.
- The below excerpt from the 2014 AHA/ACC guideline on atrial fibrillation provides a nice summary of AF in the context of critical illness.(24685669) Unfortunately, this is all that the AHA/ACC guidelines have to say about AF in the ICU – so we will have to work to fill in the blanks.
Pitfalls
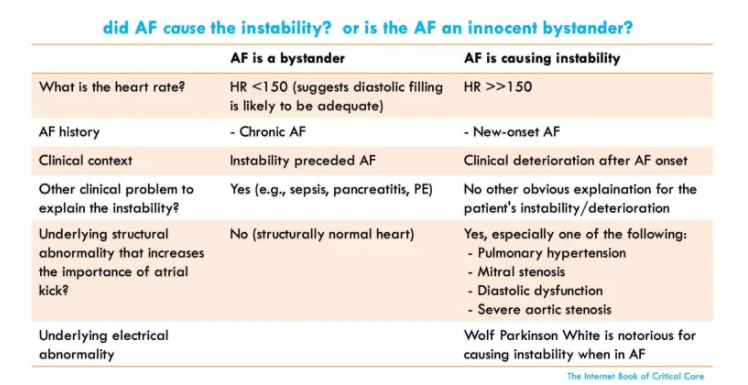
- Always look for other causes of instability among patients with AF and shock or difficulty controlling the ventricular rate. In some patients, this may be a “sinus tach equivalent” which is due to an underlying problem (e.g., sepsis, PE). In such patients, successful management depends on treating the underlying problem. Merely trying to squash the heart rate can be dangerous among these patients, as it may suppress a compensatory tachycardia.
- ACLS guidelines typically recommend immediate cardioversion for unstable patients with AF. However, among critically ill patients this has a low success rate.