Dr. Lisa Sanders’ series, Diagnosis, in the New York Times is very much worth reviewing. Follow the preceding link to a number of very interesting cases of medical detection. All physicians and nurses will find them interesting and full of clinically useful nuggets.
I’ll be looking at the article below, and others from the series in upcoming posts, from the point of view of a primary care office practioner.
The article, All Signs Pointed to a Stroke. Then the Tests Come Back Negative.
Diagnosis (By LISA SANDERS, M.D. SEPT. 26, 2017), describes the case of a 94 year old woman who presented to the emergency department with what very much appeared to be a stroke.
Her left eyelid hung lower across her eye than her right. She was seeing double, she told them. And the left side of her mouth and tongue felt strangely heavy, making it hard to speak. Initial blood tests came back normal; so did the CT scan of her brain. It wasn’t clear what was wrong with the patient, so she was transferred to nearby Yale New Haven Hospital.
Dr. Paul Sanmartin, a resident in the second year of his neurology training, met the patient early the next morning. He’d already heard about her from the overnight resident: a 94-year-old woman with the sudden onset of a droopy eyelid, double vision and difficulty speaking, probably due to a stroke.
The patient’s story was also different from what he expected. She had macular degeneration and had been getting shots in her left eye for more than a decade. Her last injection was nearly two weeks earlier, and she’d had double vision and the droopy eyelid on and off ever since.
The patient “had double vision and the droopy eyelid on and off” for two weeks just after she got a shot in her left eye for macular degeneration.
It is the intermitent TIA like symptoms above that the primary care physician is most likely to see in his or her office. And although this case turned out to be caused by myasthenia gravis, this presentation in general is far more likely to be due to a TIA or stroke.
And so the primary care practitoner seeing this patient in the office with this history and a normal physical exam, should evaluate the patient for a TIA with the aim of trying to prevent stroke.
And so I reviewed my post, 2014 Preventing Stroke In Pts With Stroke and Transient Ischemic Attack (TIA) And References That Cite The Article Posted on March 5, 2016:
The key to prevention of a future stroke when the diagnosis of transient ischemic attack (TIA)* or stroke is made is to determine the urgency of making the diagnosis by using the ABCD2 score. And then promptly obtain tests that will allow you to determine the presumed mechanism of the TIA so you can begin the appropriate preventive therapy. *TIA is a purely clinical diagnosis based on the history as the patient is normal at the time of the exam.
Studies that are relevant to the determination of the etiology of a transient ischemic attack can include a CT scan of the head without contrast (to look for intracranial bleed), an electrocardiogram (to look for arrhythmias and evidence of heart damage), CT Angiogram of the neck and intracranial vessels to look for severe vascular disease), a diffusion weighted MRI of the brain to look for previous silent cerebrovascular accidents, and other tests such as Holter, event recorder, and lab tests.
Other tests might also include a transthoracic or transesophageal echocardiogram.
The clinician can determine the urgency with which to conduct the evaluation [immediate referral to the emergency department for expedited workup or outpatient evaluation] by using the ABCD2 score, Diagnosis of Transient Ischemic Attack (TIA) Using the ABCD2 Score from the Ischemic Stroke Module of the Emergency Neurological Life Support Course Posted on September 11, 2015.
And for more help in preventive decision making review Atrial Fib + “Use of the CHA2DS2-VASc and HAS-BLED Scores to Aid Decision Making. . .” Posted on March 13, 2016
Note to myself: click on the above two link ands read both posts, both are brief and there is no point in recopying them here.
In the NYT article, all the tests for stroke and TIA were negative and it turned out that she had myasthenia gravis which is unusual in a person of her age.
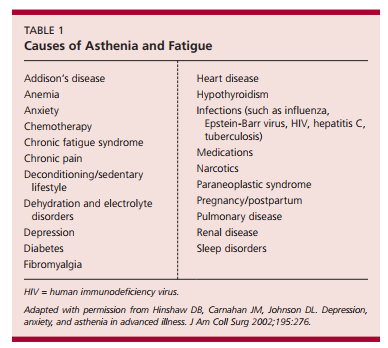
Some of the causes of generalized weakness are discussed in
Here are some clinical cases of weakness from The Differential Diagnosis of Weakness: 5 Cases December 01, 2007 from Patient Online:
- Progressive Weakness in a Woman With Systemic Lupus Erythematosus – Polymyositis
- Double Vision and Ptosis in a Young Woman With Hyperthyroidism – Myasthinia Gravis
- Progressive Numbness and Tingling in a Young Traveler – Guillain-Barre Syndrome
- Gradual Onset of Hand Weakness in a Healthy Man – Amyotrophic Lateral Sclerosis
- Student With Weakness and Numbness – Multiple Sclerosis
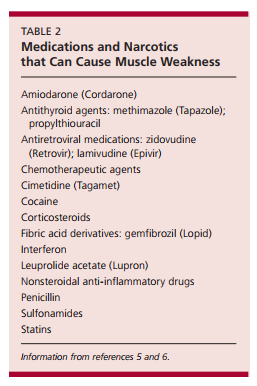
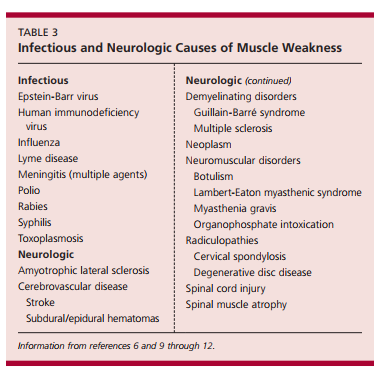
An excellent article on the subject from American Family Physician is Evaluation of the patient with muscle weakness [PubMed Abstract]. Am Fam Physician. 2005 Apr 1;71(7):1327-36. Here are three tables from the article: