The Edmonton Symptom Assessment Scale is a very useful instrument.
Although the scale is designed for symptom assessment in cancer patients, many clinicians may find it useful in other patients.
Here are Guidelines for using the Edmonton Symptom Assessment System (ESAS) [PDF]:
Purpose of the ESAS
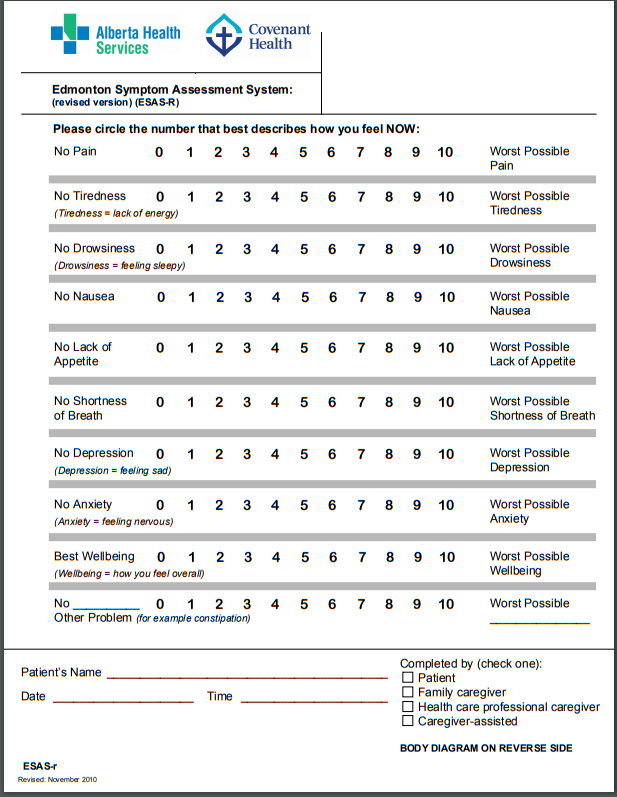
This tool is designed to assist in the assessment of nine symptoms common in cancer patients: pain, tiredness, nausea, depression, anxiety, drowsiness, appetite, wellbeing and shortness of breath, (there is also a line labelled “Other Problem”). The severity at the time of assessment of each symptom is rated from 0 to 10 on a numerical scale, 0 meaning that the symptom is absent and 10 that it is of the worst possible severity. The patient and family should be taught how to complete the scales. It is the patient’s opinion of the severity of
the symptoms that is the “gold standard” for symptom assessment. The ESAS provides a clinical profile of symptom severity over time. It provides a context within which
symptoms can begin to be understood. However, it is not a complete symptom assessment in itself. For good symptom management to be attained the ESAS must be used as just one part of a holistic clinical assessment.How to do the ESAS
The patient circles the most appropriate number to indicate where the symptom is between the two extremes.No pain 0 1 2 3 4 5 6 7 8 9 10 Worst possible pain
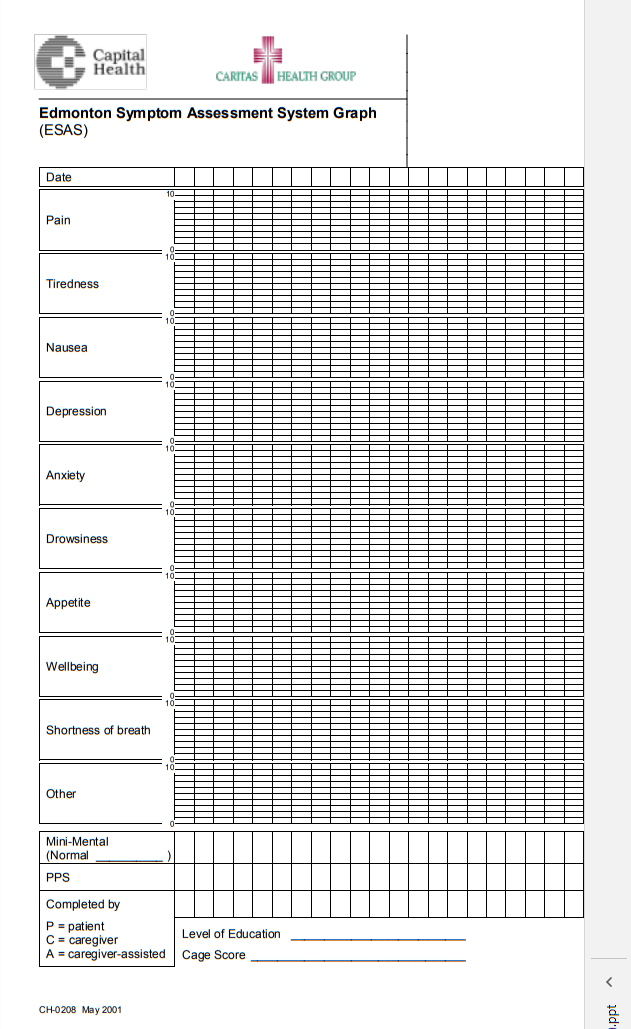
The circled number is then transcribed onto the symptom assessment graph (see “ESAS Graph” below).
Synonyms for words that may be difficult for some patients to comprehend include the following:
Depression – blue or sad
Anxiety – nervousness or restlessness
Tiredness – decreased energy level (but not necessarily sleepy)
Drowsiness – sleepiness
Wellbeing – overall comfort, both physical and otherwise; truthfully answering the question, “How are you?”When to do the ESAS
a) In palliative home care, it is a good practice to complete and graph the ESAS during each telephone or personal contact. If symptoms are in good control, and there are no predominant psychosocial issues, the ESAS can be completed weekly for patients in the home. In hospice and tertiary palliative care units the ESAS should be completed daily. In other settings the palliative consultants will utilize this tool in their assessment on
each visit.
b) If the patient’s symptoms are not in good control, daily assessments need to be done in person by the
attending health professionals until the symptoms are well-controlled (see “d” below).
c) If symptom management is not attained, or consultation about possible care options is needed, patient
assessments by Palliative Care Consultants are available (attending physician must agree). Consultative
discussions not requiring in-person patient assessments are available from Palliative Care Consultants upon
request.
d) If, after all therapeutic options have been exhausted and consensus is reached that a symptom cannot be
further improved, visits and assessments can return to their normal pattern for that patient.Who should do the ESAS
Ideally, patients fill out their own ESAS. However, if the patient is cognitively impaired or for other reasons cannot independently do the ESAS, then it is completed with the assistance of a caregiver (a family member, friend, or health professional closely involved in the patient’s care). If the patient cannot participate in the symptom assessment, or refuses to do so, the ESAS is completed by the caregiver alone.
Note: when the ESAS is completed by the caregiver alone the subjective symptom scales are not done (i.e. tiredness, depression, anxiety, and wellbeing are left blank) and the caregiver assesses the remaining symptoms as objectively as possible, i.e. pain is assessed on the basis of a knowledge of pain behaviors, appetite is interpreted as the absence or presence of eating, nausea as the absence or presence of retching or
vomiting, and shortness of breath as laboured or accelerated respirations that appears to be causing distress for the patient.
When a patient is irreversibly cognitively impaired and cannot participate in doing the ESAS, the caregiver
continues to complete the ESAS as outlined above and the Edmonton Comfort Assessment Form (ECAF) may also be used (see ECAF guidelines). The method in which the ESAS was completed must be indicated in the space provided at the bottom of the ESAS Numerical Scale and the ESAS GraphWhere to document the ESAS
The ESAS is always done on the ESAS Numerical Scale and the results later transferred to the ESAS
Graph. Graphing symptom severity directly onto the ESAS Graph without the use of the numerical scale is not
a valid use of the ESAS nor a reliable method of symptom assessment (attention to the graphed historical
trend may affect the current scores and so undermine one of the main purposes of the ESAS, i.e. to assess the
current symptom profile as accurately as possible).Other Information About the ESAS
The ESAS Graph also contains space to add the patient’s Mini-Mental Status Exam score. The “normal” box
refers to the normal range for the patient, based on age and education level (see Instructions for MMSE). As
well, a space for the Palliative Performance Scale (PPS) is included. The ESAS is available in other
languages and also in faces for those patients who do not read.