
In this post, I link to and excerpt from Development and Validation of a Novel Pediatric Appendicitis Risk Calculator (pARC) [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Pediatrics. 2018 Apr;141(4):e20172699.
The above article was cited by 13 articles in PubMed.
There were 61 similar articles in PubMed in the last five years.
All that follows is from the above resource.
Abstract
Objectives: We sought to develop and validate a clinical calculator that can be used to quantify risk for appendicitis on a continuous scale for patients with acute abdominal pain.
Methods: The pediatric appendicitis risk calculator (pARC) was developed and validated through secondary analyses of 3 distinct cohorts. The derivation sample included visits to 9 pediatric emergency departments between March 2009 and April 2010. The validation sample included visits to a single pediatric emergency department from 2003 to 2004 and 2013 to 2015. Variables evaluated were as follows: age, sex, temperature, nausea and/or vomiting, pain duration, pain location, pain with walking, pain migration, guarding, white blood cell count, and absolute neutrophil count. We used stepwise regression to develop and select the best model. Test performance of the pARC was compared with the Pediatric Appendicitis Score (PAS).
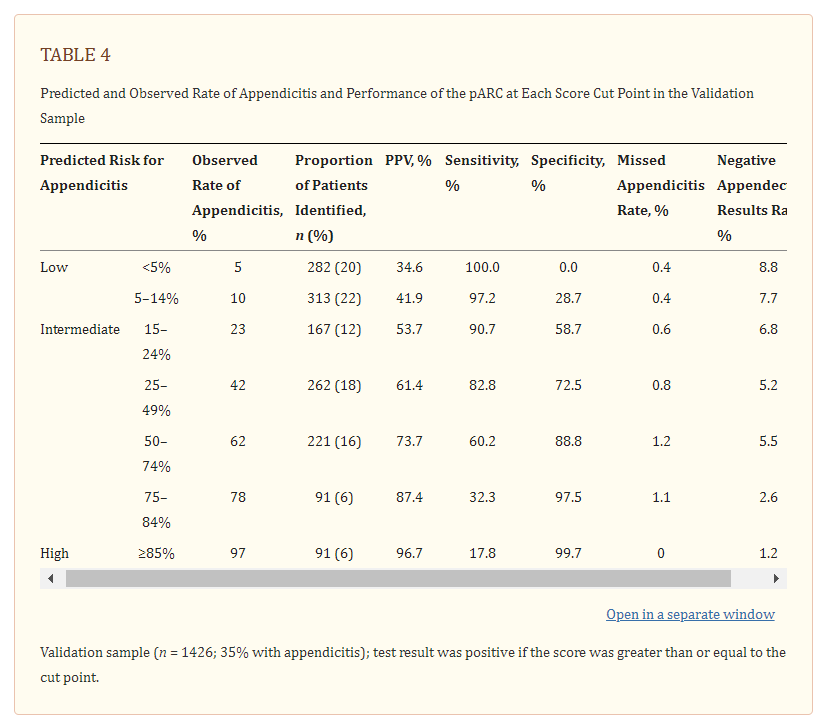
Results: The derivation sample included 2423 children, 40% of whom had appendicitis. The validation sample included 1426 children, 35% of whom had appendicitis. The final pARC model included the following variables: sex, age, duration of pain, guarding, pain migration, maximal tenderness in the right-lower quadrant, and absolute neutrophil count. In the validation sample, the pARC exhibited near perfect calibration and a high degree of discrimination (area under the curve: 0.85; 95% confidence interval: 0.83 to 0.87) and outperformed the PAS (area under the curve: 0.77; 95% confidence interval: 0.75 to 0.80). By using the pARC, almost half of patients in the validation cohort could be accurately classified as at <15% risk or ≥85% risk for appendicitis, whereas only 23% would be identified as having a comparable PAS of <3 or >8.
Conclusions: In our validation cohort of patients with acute abdominal pain, the pARC accurately quantified risk for appendicitis.
The pARC and Ultrasound
In Table 5, we present the relationship between the pARC strata, ultrasound use, and performance of ultrasound. Of 2423 subjects in our derivation sample, 905 (37%) had an ultrasound, with use being the highest in the 2 lowest pARC strata (45% for pARC scores of <5% risk and 46% for pARC scores of 5% to 14% risk). Overall, 443 (49%) of patients who underwent an ultrasound had an equivocal study, and the rate of appendicitis after an equivocal ultrasound was 18%. The PPV of ultrasound was ≤70% for patients with a pARC score of <25%. For pARC risk strata of 25% or higher, the PPV of ultrasound increased to ≥94%.
Discussion
In this large multicenter study, we have demonstrated that the newly derived and validated pARC can be used to provide an accurate and discrete assessment of a patient’s risk for appendicitis, with improved accuracy and clinical use as compared with a previously published appendicitis score. Importantly, in our validation cohort with a background risk of appendicitis of 35%, the pARC score was able to classify half of patients as at ≥85% risk or <15% risk for appendicitis, thresholds where surgical evaluation or observation, respectively, may be recommended over immediate diagnostic imaging.
Advanced diagnostic imaging remains common for patients with suspected appendicitis,28 with upwards of 80% undergoing ultrasound, CT, or MRI.29 . . . Despite the high use, the type of diagnostic imaging has shifted dramatically over the past decade, with Bachur et al6 reporting a 48% decline in CT use from 2010 to 2013 for patients with appendicitis across 35 children’s hospitals. During this period, the use of ultrasound increased 46%, and overall imaging rates remained unchanged.6
The decline in use of CT is significant because fewer children are exposed to ionizing radiation.32 However, the high use of ultrasound raises the potential for overuse. . . . In some centers, half of ultrasounds are reported as equivocal33; these equivocal ultrasounds may compel providers to order a CT, MRI, or admit for observation.34 This is especially concerning in cases in which the a priori risk for appendicitis is low and highlights the need for judicious, risk-stratified use of any diagnostic imaging.
The use of diagnostic imaging for patients with acute abdominal pain may be magnified when patients are assigned intermediate appendicitis risk scores. It is in this context that the pARC may be most impactful on clinical care. In our study, up to 40% of the pediatric patients who presented with acute abdominal pain would have been assigned a low risk pARC score by which the clinician could defer diagnostic imaging. Furthermore, in the subset assigned a pARC score of 15% to 24%, the high rate of equivocal ultrasound readings and ultimate low risk for appendicitis suggests that these patients may be managed with observation rather than ultrasound. Finally, among patients with pARC scores ≥85%, it would be reasonable and safe to encourage surgical evaluation with selective use of diagnostic imaging. The potential implications of this approach merit discussion among multidisciplinary care teams. Suggested in the data presented here is that broad use of the pARC score at the point of care could facilitate a reduction in the use of ultrasound, CT, and MRI.
One strength of our study lies in the approach used to develop the pARC, because it differed substantially from methods used in the derivation of previous appendicitis risk scores.
Several limitations should be noted. First, a few variables we considered for inclusion had substantial missing data and could not be incorporated in the model. Second, the pARC was derived and validated by using data from patients at children’s hospitals. Furthermore, for the validation cohort, we aggregated data from different time periods from a single children’s hospital. As such, our results require validation in new populations before widespread dissemination. Similarly, our derivation and validation cohorts had appendicitis at rates of 40% and 35%, respectively. The discriminative power of the pARC may be diminished if applied in populations with higher or lower appendicitis rates.* In addition, the pARC is not intuitive and requires sophisticated calculations. Nevertheless, the pARC can be easily programmed and integrated within the electronic health record, promoting meaningful use of available clinical and laboratory data.

*See Validation of the Pediatric Appendicitis Risk Calculator (pARC) in a Community Emergency Department Setting [PubMed Abstract]. Ann Emerg Med. 2019 Oct;74(4):471-480.



