This year I’ll be renewing my ACLS, PALS, and NRC certifications. Hopefully, I’ll get to attend an in-person class [I get as much out of interacting with my fellow students as I do from studying the course materials]. But most likely, the courses will take place online.
What follows are my study notes and readers of the blog should just go to the Highlights as these excerpts are in no way a substitute for that awesome resource.
In this post I link to and excerpt from the section on Adult Basic and Advanced Life Support section of Highlights Of The 2020 American Heart Association For CPR And ECC [Link is to the PDF].
Here are excerpts:
Introduction
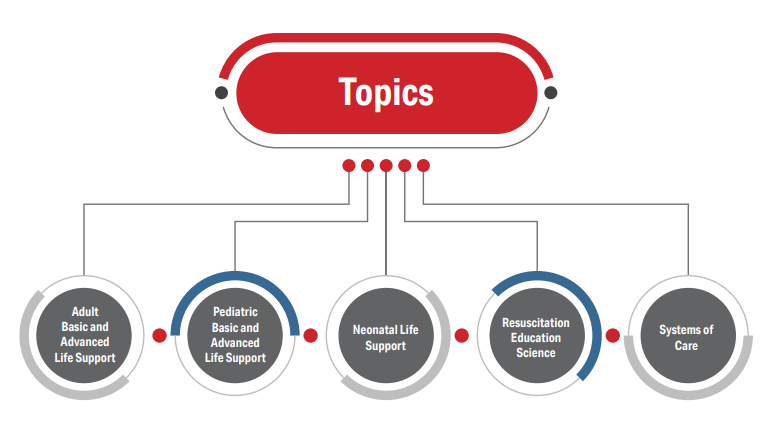
These Highlights summarize the key issues and changes in the 2020 American Heart Association (AHA) Guidelines for
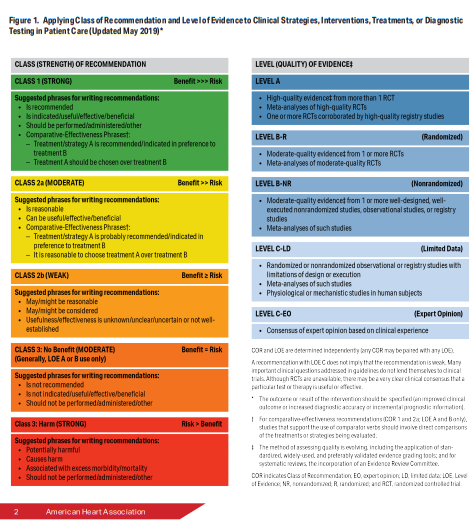
Cardiopulmonary Resuscitation (CPR) and Emergency Cardiovascular Care (ECC). The 2020 Guidelines are a comprehensive revision of the AHA’s guidelines for adult, pediatric, neonatal, resuscitation education science, and systems of care topics.The 2020 Guidelines use the most recent version of the AHA definitions for the COR and LOE (Figure 1).
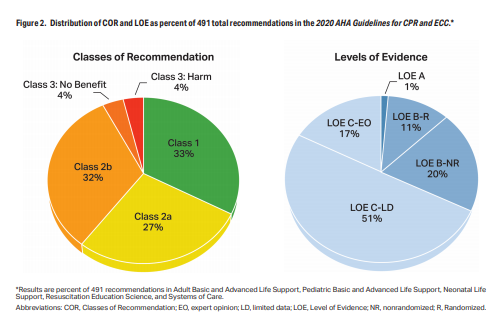
Overall, 491 specific recommendations are made for adult, pediatric, and neonatal life support; resuscitation education science; and systems of care. Of these recommendations, 161 are class 1 and 293 are class 2 recommendations (Figure 2). Additionally, 37 recommendations are class 3, including 19 for evidence of no benefit and 18 for evidence of harm.
Adult Basic and Advanced Life Support
Summary of Key Issues and Major Changes
In 2015, approximately 350 000 adults in the United States
experienced nontraumatic out-of-hospital cardiac arrest
(OHCA) attended by emergency medical services (EMS)
personnel. Despite recent gains, less than 40% of adults
receive layperson-initiated CPR, and fewer than 12% have
an automated external defibrillator (AED) applied before EMS
arrival. After significant improvements, survival from OHCA
has plateaued since 2012.In addition, approximately 1.2% of adults admitted to US
hospitals suffer in-hospital cardiac arrest (IHCA). Outcomes
from IHCA are significantly better than outcomes from OHCA,
and IHCA outcomes continue to improve.Recommendations for adult basic life support (BLS) and
advanced cardiovascular life support (ACLS) are combined
in the 2020 Guidelines. Major new changes include the
following:
• Enhanced algorithms and visual aids provide easy-to remember guidance for BLS and ACLS resuscitation
scenarios.
• The importance of early initiation of CPR by lay rescuers
has been re-emphasized.
• Previous recommendations about epinephrine
administration have been reaffirmed, with emphasis on
early epinephrine administration.
• Use of real-time audiovisual feedback is suggested as a
means to maintain CPR quality.
• Continuously measuring arterial blood pressure and endtidal carbon dioxide (ETCO2) during ACLS resuscitation
may be useful to improve CPR quality.
• On the basis of the most recent evidence, routine use of
double sequential defibrillation is not recommended.
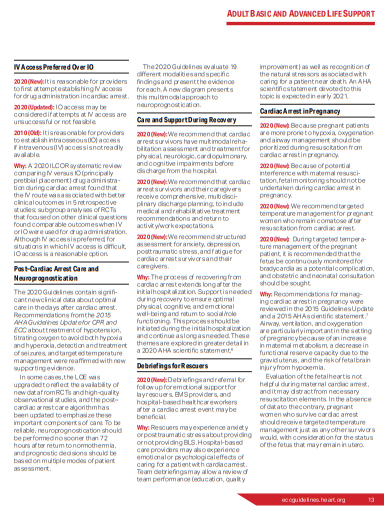
• Intravenous (IV) access is the preferred route of medication
administration during ACLS resuscitation. Intraosseous (IO)
access is acceptable if IV access is not available.
• Care of the patient after return of spontaneous circulation
(ROSC) requires close attention to oxygenation, blood pressure control, evaluation for percutaneous coronary
intervention, targeted temperature management, and
multimodal neuroprognostication.
• Because recovery from cardiac arrest continues long
after the initial hospitalization, patients should have formal
assessment and support for their physical, cognitive, and
psychosocial needs.
• After a resuscitation, debriefing for lay rescuers, EMS
providers, and hospital-based healthcare workers may be
beneficial to support their mental health and well-being.
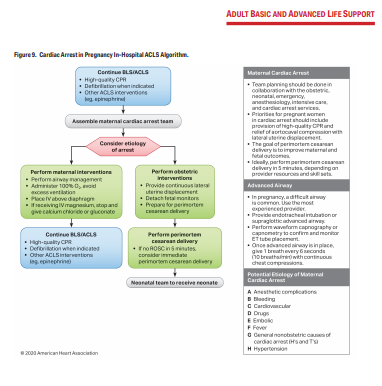
• Management of cardiac arrest in pregnancy focuses on
maternal resuscitation, with preparation for early perimortem
cesarean delivery if necessary to save the infant and
improve the chances of successful resuscitation of
the mother.Algorithms and Visual Aids
The writing group reviewed all algorithms and made focused
improvements to visual training aids to ensure their utility as
point-of-care tools and reflect the latest science. The major
changes to algorithms and other performance aids include
the following:
• A sixth link, Recovery, was added to the IHCA and OHCA
Chains of Survival (Figure 3).
• The universal Adult Cardiac Arrest Algorithm was modified
to emphasize the role of early epinephrine administration for
patients with nonshockable rhythms (Figure 4).
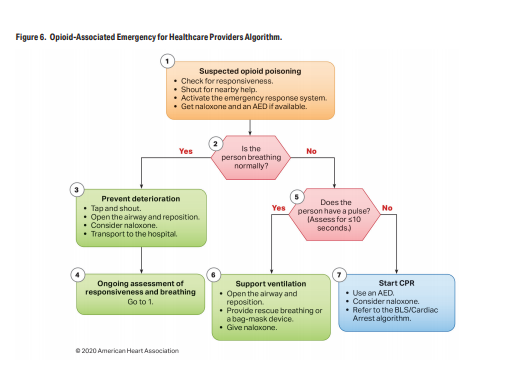
• Two new Opioid-Associated Emergency Algorithms have
been added for lay rescuers and trained rescuers
(Figures 5 and 6).
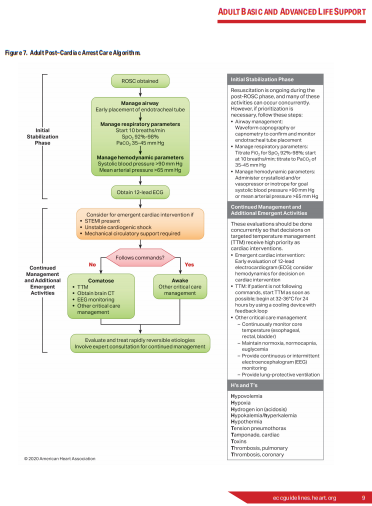
• The Post–Cardiac Arrest Care Algorithm was updated to
emphasize the need to prevent hyperoxia, hypoxemia, and
hypotension (Figure 7).
• A new diagram has been added to guide and inform
neuroprognostication (Figure 8).
• A new Cardiac Arrest in Pregnancy Algorithm has been
added to address these special cases (Figure 9).




Major New and Updated Recommendations
Early Initiation of CPR by Lay Rescuers
2020 (Updated): We recommend that laypersons initiate CPR for presumed cardiac arrest because the risk of harm to the patient is low if the patient is not in cardiac arrest.
2010 (Old): The lay rescuer should not check for a pulse and should assume that cardiac arrest is present if an adult
suddenly collapses or an unresponsive victim is not breathing normally. The healthcare provider should take no more than 10 seconds to check for a pulse and, if the rescuer does not definitely feel a pulse within that time period, the rescuer should start chest compressions.Why: New evidence shows that the risk of harm to a victim who receives chest compressions when not in cardiac
arrest is low. Lay rescuers are not able to determine with accuracy whether a victim has a pulse, and the risk of withholding CPR from a pulseless victim exceeds the harm from unneeded chest compressions.Early Administration of Epinephrine
2020 (Unchanged/Reaffirmed): With respect to timing, for cardiac arrest with a nonshockable rhythm, it is
reasonable to administer epinephrine as soon as feasible.2020 (Unchanged/Reaffirmed): With respect to timing, for cardiac arrest with a shockable rhythm, it may be reasonable to administer epinephrine after initial defibrillation attempts have failed.
Why: The suggestion to administer epinephrine early was strengthened to a recommendation on the basis of a systematic review and meta-analysis, which included results of 2 randomized trials of epinephrine enrolling more than 8500 patients with OHCA, showing that epinephrine increased ROSC and survival. At 3 months, the time point felt to be most meaningful for neurologic recovery, there was a nonsignificant increase in survivors with both favorable and unfavorable neurologic outcome in the epinephrine group.
Of 16 observational studies on timing in the recent systematic review, all found an association between earlier epinephrine and ROSC for patients with nonshockable rhythms, although improvements in survival were not universally seen. For patients with shockable rhythm, the literature supports prioritizing defibrillation and CPR initially and giving epinephrine if initial attempts with CPR and defibrillation are not successful.
Any drug that increases the rate of ROSC and survival but is given after several minutes of downtime will likely increase both favorable and unfavorable neurologic outcome. Therefore, the most beneficial approach seems to be continuing to use a drug that has been shown to increase survival while focusing broader efforts on shortening time to drug for all patients; by doing so,
more survivors will have a favorable neurologic outcome.Real-Time Audiovisual Feedback
2020 (Unchanged/Reaffirmed): It may be reasonable to use audiovisual feedback devices during CPR for real-time optimization of CPR performance.
Why: A recent RCT reported a 25% increase in survival to hospital discharge from IHCA with audio feedback on compression depth and recoil.
Physiologic Monitoring of CPR Quality
2020 (Updated): It may be reasonable to use physiologic parameters such as arterial blood pressure or ETCO2 when
feasible to monitor and optimize CPR quality.2015 (Old): Although no clinical study has
examined whether titrating resuscitative efforts to physiologic parameters during CPR improves outcome, it may be reasonable to use physiologic parameters (quantitative waveform capnography, arterial relaxation diastolic pressure, arterial pressure monitoring, and central venous oxygen saturation) when feasible to monitor and optimize CPR quality, guide vasopressor therapy, and detect ROSC.Why: Although the use of physiologic monitoring such as arterial blood pressure and ETCO2 to monitor CPR
quality is an established concept, new data support its inclusion in the guidelines. Data from the AHA’s Get With The Guidelines®-Resuscitation registry show higher likelihood of
ROSC when CPR quality is monitored using either ETCO2 or diastolic blood pressure.This monitoring depends on the presence of an endotracheal tube (ETT) or arterial line, respectively. Targeting compressions to an ETCO2 value of at least 10 mm Hg, and ideally 20 mm Hg
or greater, may be useful as a marker of CPR quality. An ideal target has not been identified.Double Sequential Defibrillation Not Supported
2020 (New): The usefulness of double sequential defibrillation for refractory shockable rhythm has not been established.
Why: Double sequential defibrillation is the practice of applying near simultaneous shocks using 2 defibrillators. Although some case reports have shown good outcomes, a 2020 ILCOR systematic review found no evidence to support double sequential defibrillation and recommended against its routine use. Existing studies are subject to multiple forms of bias,
and observational studies do not show improvements in outcome.A recent pilot RCT suggests that changing the direction of defibrillation current by repositioning the pads may be as effective as double sequential defibrillation while avoiding the risks of harm from increased energy and damage to defibrillators. On the basis of current evidence, it is not known
whether double sequential defibrillation is beneficial.
Start at below