
In this post I link to and excerpt from Emergency Medicine Cases’ ECG Cases 9 – First Diagonal Occlusion. Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman, May 2020.
All that follows is from Dr. McLaren’s post.
In this ECG Cases blog we look at 6 patients who presented with potentially ischemic symptoms, “STEMI negative” but signs of a specific coronary occlusion.
Six patients presented with ischemic symptoms, “STEMI negative”.
First diagonal occlusion
STEMI is defined as ST elevation in two contiguous leads of at least 1mm (and greater in V2-3 based on age/sex), in the absence of LVH or LBBB. However, an occlusion of the first diagonal branch of the left anterior descending artery (LAD), which runs diagonally over the left ventricle to supply its anterolateral wall, often defies this classification. The resulting missed MIs are often associated with poorer outcomes. Although they are traditionally considered noncontiguous leads, ST elevations in aVL and V2 (with concurrent inferior ST depressions) should prompt a consideration of diagonal branch occlusion.[1]
This pattern was recognized 25 years ago, and differentiated from other occlusions that can cause ST elevation in aVL: “ST-segment elevation in lead aVL during AMI indicates either proximal LAD artery, Diagonal, or Obtuse Marginal [branch of circumflex] occlusion. If ST-segment elevation is found in aVL and the precordial leads V2 through V5, the culprit lesion is most probably located in the proximal portion of the LAD artery before the origin of the first diagonal branch. ST-segment elevation in leads aVL and V2, accompanied by either isoelectric or depressed ST segment in leads V3 through V6, favors occlusion of the first diagonal branch. ST elevation in aVL accompanied by isoelectric or negative ST segment in the precordial leads, including V2, predicts obstruction of the first obtuse marginal branch.” [2]
When first diagonal branch occlusion causes ST elevation in I, aVL and V2 along with inferior ST depression, it has been called the “South African flag sign“: The distribution of ST-segment deviation resembles the pattern of the South African flag with ST elevation in the upper left panel (lead I) and in the two middle panels in the second and third columns (leads aVL and V2, respectively), and ST depression in the bottom left panel (lead III). [3] Learning this classic pattern can help identify more subtle cases of first diagonal occlusion (or occasionally LAD occlusion, depending on coronary anatomy). While ST elevation in I and aVL will potentially meet classic STEMI criteria, diagonal occlusion will often not meet STEMI criteria–because the ST elevation involves noncontiguous leads aVL and V2, and/or because the degree of elevation is subtle and other signs of occlusion are needed to make the diagnosis (like new Q waves, pseudonormalized or hyperacute T waves, reperfusion T wave inversion, or reciprocal changes). First diagonal occlusion therefore serves as another reason for a paradigm shift from ST elevation MI (STEMI) to Occlusion MI (OMI).
In this ECG Cases blog we look at 6 patients who presented with potentially ischemic symptoms, “STEMI negative” but signs of a specific coronary occlusion.
Patient 1: 50yo with 5 hours of chest pain
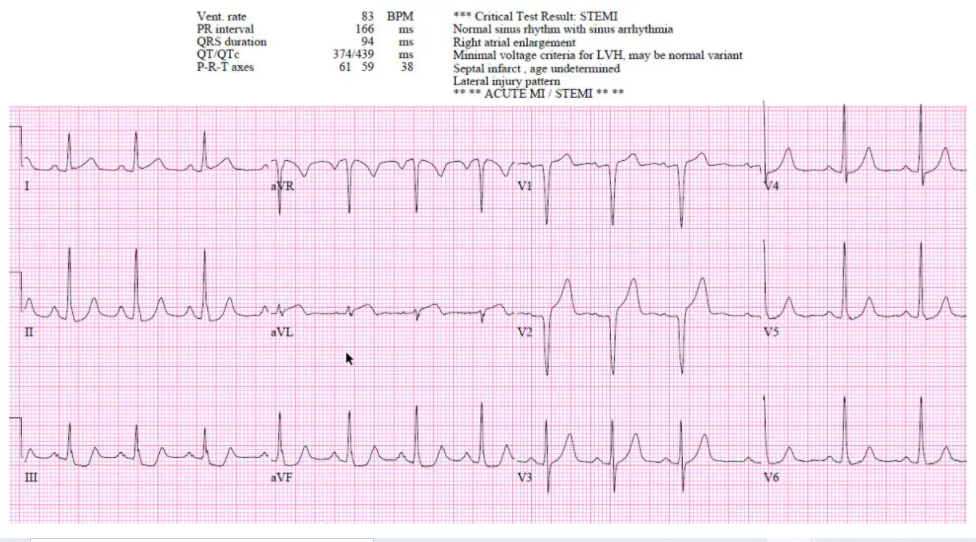
Patient 1: borderline STEMI(+), clear OMI(+) from diagonal occlusion
- Heart rate/rhythm: NSR
- Electrical conduction: normal intervals
- Axis: normal
- R-wave height/transition: normal except for Q wave in V1-V2
- Tension: LVH
- ST/T waves: borderline ST elevation V1-2, in the context of LVH. But there are hyperacute T waves in aVL/V2 and straightening of ST in I, along with inferior ST depression
Not clear STEMI but physician was concerned about aVL/V2 so stat cardiology consult. Cath lab activated: first diagonal occlusion. Discharge ECG had reperfusion T wave inversion in I, aVL and V2



