
Note to myself: In addition to Dr. Farkas’ chapter and podcast linked below, be sure to review the five posts I’ve listed below – It doesn’t take that long:
- Serotonin Syndrome – Help From Emergency Physician Educators
Posted on August 14, 2017 by Tom Wade MD - Vilazodone – Be Afraid (Be Very Afraid) – A Warning From Tox And The Hound
Posted on July 18, 2018 by Tom Wade MD- The above post contains excerpts from the outstanding from Tox and Hound – Don’t Pick the Scab – Vilazodone an SSRI with partial agony properties. July 9, 2018 from Tox & Hound by Dr. Dan Rosniak. But the Tox and Hound post is a wonderful review of how SSRIs work and should be completely rereviewed. My post just has excerpts from the above about why Vilazodone is dangerous to children.
- The DIMS Mnemonic In Fever and Altered Mental Status – “Best Case Ever 64 Salicylate Poisoning” – And Some Additional Resources
Posted on December 31, 2017 - Causes of Pediatric Agitation – Help From Pediatric EM Morsels
Posted on November 4, 2017 by Tom Wade MD - The Acutely Agitated Patient – What To Do – Help From Dr. Reuben Streyer
Posted on May 11, 2017 by Tom Wade MD
Here is the link to Dr. Farkas‘ outstanding (as always) “IBCC chapter & cast: Serotonin Syndrome” published June 13, 2019. Here is a link to the Table Of Contents of The Internet Book Of Critical Care [If you haven’t visited this link, then explore it now. It is an awesome resource].
Here is the intro to IBCC chapter & cast: Serotonin Syndrome:
Serotonin syndromes comes up a lot in critical care medicine. Sometimes we are admitting patients because of a primary diagnosis of serotonin syndrome. Other times we are afraid of causing serotonin syndrome ourselves, due to polypharmacy. In both scenarios, there may be uncertainty regarding whether or not a patient has serotonin syndrome.
This chapter explores the causes, presentation, and treatment of serotonin syndrome. There are precisely zero human RCTs on the treatment of serotonin syndrome, so this leaves considerable room for debate. A treatment algorithm is proposed which I believe is reasonable (while fully acknowledging that there are numerous other potential strategies to treat this disease and no conclusive evidence regarding which is best).
- The IBCC chapter is located here.
And here are direct links to the Contents of this IBCC chapter. Each link will jump directly to that section of this IBCC chapter [I put the following in because these posts are my medical study notes]:
CONTENTS
And here are excerpts from IBCC chapter and cast: Serotonin syndrome:
overview
- Serotonin syndrome usually results from inadvertent interaction of several serotonergic medications.
- Most cases are mild-moderate, and will improve in about a day following cessation of medications. However, serotonin syndrome can be severe and may require ICU admission.
- The main challenge is recognition: If serotonin syndrome is recognized early and causative drugs are stopped immediately, then patients will generally do very well.
clinical presentation
- Usually occurs promptly following medication exposure or dose adjustment (within 12-24 hours).
- Will generally resolve within 24 hours following discontinuation of causitive medications.
- Rapid onset & resolution can be helpful diagnostically to distinguish from many other disorders (e.g. neuroleptic malignant syndrome, thyrotoxicosis).
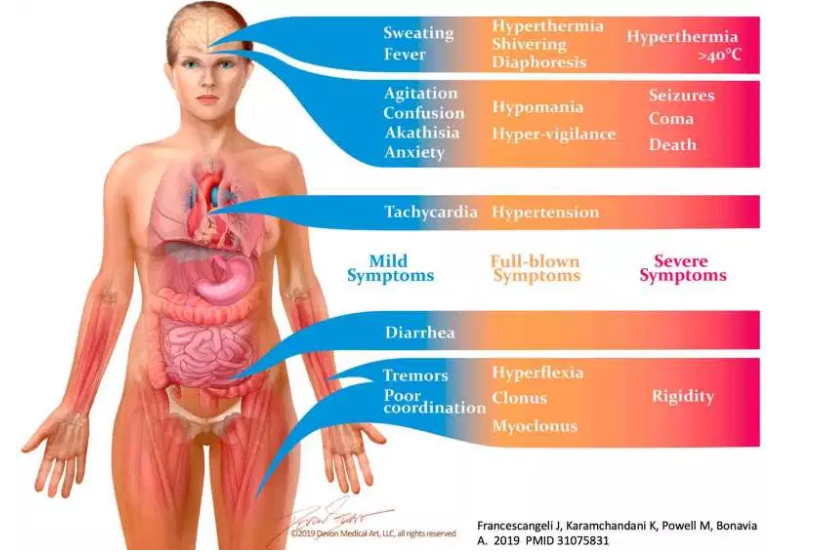
overall presentation: triad of findings
- (1) Mental status change
- Anxiety, agitated delirium
- Seizure, coma
- (2) Sympathetic hyperactivity
- hyperthermia
- hypertension, tachycardia
- diaphoresis, flushing
- mydriasis
- Nausea/vomiting, diarrhea (may occur early, as a prodrome)
- (3) Neuromuscular excitation
- Hyperreflexia
- Clonus
- Most common: elicited by dorsiflexion of foot
- Ocular clonus (ping-pong gaze)
- Spontaneous clonus in most severe cases (can mimic seizure)
- Tremor
- Rigidity (one of the most severe and dangerous manifestation)
- Akathisia (inability to stay still)
differential diagnosis
The differential diagnosis will depend on the particular presenting symptoms. The following are the most common considerations:
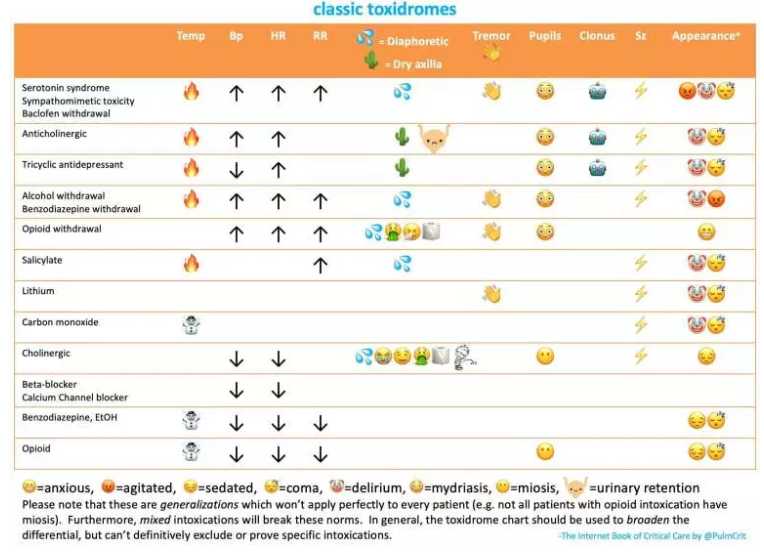
other toxidromes (usually the closest mimics)
- Serotonin syndrome can be indistinguishable from sympathomimetic intoxication (and these may be largely the same thing, because sympathomimetics increase serotonin levels)
- Alcohol or baclofen withdrawal.
- Anticholinergic toxicity
sepsis
- Serotonin syndrome can be a sepsis mimic (e.g. can cause fever, elevated lactate, tachycardia).
- Meningitis or encephalitis may look a lot like serotonin syndrome.
hyperthermia syndromes
- Neuroleptic malignant syndrome
- Malignant hyperthermia
- Brainstem stroke causing hyperthermia
- Heat stroke
other
- Thyrotoxicosis
- Sympathetic Storm
lab evaluation
Labs don’t help diagnose serotonin syndrome. However, they may be useful in excluding alternative diagnoses and in evaluating complications of serotonin syndrome.
lab abnormalities may include:
- Leukocytosis
- Lactic acidosis
- Elevated creatine kinase (rhabdomyolysis)
- Disseminated intravascular coagulation
- Renal failure
- Liver function abnormalities
- Hyponatremia, hypomagnesemia
tests to consider (evaluation depends on presentation, but consider the following)
- EKG
- Labs
- Fingerstick glucose
- Chemistries, including Ca/Mg/Phos
- Creatinine kinase
- Liver function tests
- Coagulation studies
- Salicylate & acetaminophen levels
- Infectious workup (blood & urine cultures)
- CSF analysis if concern for meningitis/encephalitis
- Imaging
- Chest X-ray
- CT head, possibly MRI
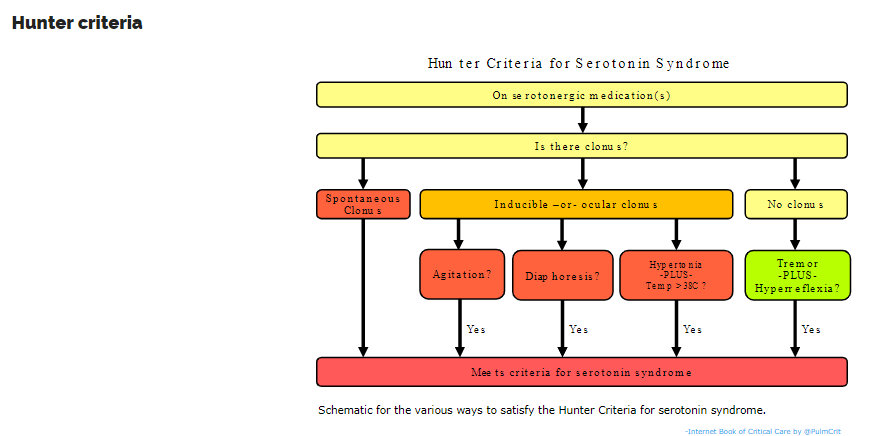
diagnostic criteria
- Among various criteria, the Hunter Criteria seem to be the best. Compared to evaluation by a medical toxicologist, these criteria are 84% sensitive and 97% specific.
- Of course, rigid application of criteria should never supersede clinical judgement.
- These criteria rightfully place clonus at the center of the diagnosis (as discussed above).
- Defining precisely whether or not a patient has serotonin syndrome is tough because this is a spectrum disorder which ranges from mild to severe. Very mild serotonin syndrome might not meet the Hunter Criteria (which are more specific than sensitive).
Please see the IBCC chapter & cast: Serotonin Syndrome for an outstanding video from the New England Journal of Medicine demonstrating Ocular Clonus.
Treatment
basic principles of treatment
- Key principles:
- (1) The natural history of serotonin syndrome is that once causative medications are stopped, patients will improve rapidly (usually within a day). Most patients don’t require anything more than high-quality supportive care. All you need to do is stop the offensive drugs and keep the patients safe, and they will recover.
- (2) The pathway whereby serotonin syndrome leads to death is hyperthermia. Hyperthermia may promote seizures, leading to a seizure-coma-death spiral.
- Primary goals of treatment:
- (1) Monitor temperature and treat/avoid hyperthermia.
- (2) Treat agitation as needed to keep patient comfortable.
hyperthermia control*
- Key treatments:
- (1) Hyperthermia needs to be controlled with physical cooling techniques (e.g. cooling blanket, Arctic Sun, fan).
- (2) Agitation should be controlled as discussed above, to prevent muscular activity that could worsen hyperthermia.
- Antipyretics won’t work (these patients don’t have hypothalamically mediated fever).
- For extreme hyperthermia (e.g. temperature over ~41.1 C), intubation with non-depolarizing paralysis may be considered as the fastest way to control temperature (24358002).
*See Resources (1) and (2) in Additional Resources below for more on the treatment of severe hyperthermia.
intubation
- May occasionally be required for the following reasons:
- (1) In extreme cases, chest wall rigidity may interfere with ventilation
- (2) Profound hyperthermia
- (3) Uncontrollable agitation
- (4) Status epilepticus
- Paralysis may be useful initially (especially in the case of profound hyperthermia).
rhabdomyolysis
- It this occurs, treat as described in the chapter on rhabdomyolysis.
Additional Resources:
(1) Cooling Techniques for Hyperthermia from emedicine.medscape.com
Updated: May 14, 2018 Author: Erik D Schraga, MD
(2) Cooling Techniques For Hyperthermia from StatPearls
Deena D. Wasserman; Megan Healy. Last Update: February 10, 2019.



