
In this post I link to and excerpt from Life In The Fast Lane‘s outstanding ECG Exam Template by Chris Nickson Feb 4, 2021.
Note to my readers: Readers should just go to the link above to review the template. I recopy and post excerpts because it helps me to fix the information in my mind (like high-lighting print text in the pre-internet days). And as you go through Dr. Nickson’s post, be sure to review every link in the post. They are all critical.<– Note to myself also.
And for more great ECG learning resources from LITFL, see The ECG Basics Home Page.
All that follows is from the above post.
The following headings and prompts can be used as template for ECG-based exam questions.
ECG type and recording
- 12 lead vs rhythm strip, rate (normal 25 mm/s)
- Calibration (5mm wide, 10mm high = 1mV)
- Unusual leads – right, posterior, lead grouping format
Rate
- normal 60 – 100/min
- tachy/bradycardia (SA node) vs –arrhythmia (not SA node)
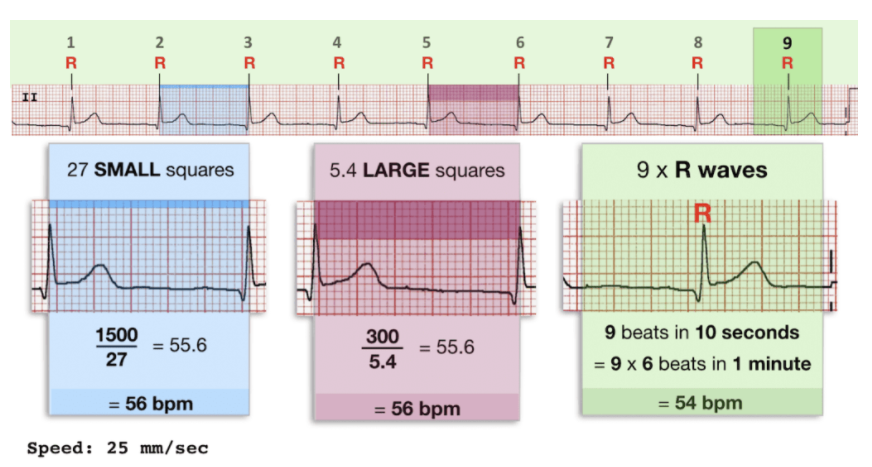
- method: 300/RR interval (large squares) or number of QRS complexes x 6 (if 25mm/s)
Rhythm
- Pattern – regular/ regularly irregular/ irregularly irregular
- Seven step approach to rhythm analysis
Axis
Axis Methods:
- Quick look test (Lead I and aVF)
- Three Lead Analysis (Lead I, Lead II, aVF)
- Isoelectric Lead Analysis
- Super SAM the axis Man
PR interval + PR segment
- Duration 0.12-0.2s normal/ short/ long/ varying
- Heart blocks:
- PR depression
Q wave
- Normal: <25%R in I, aVL, AVF, V456
- Pathological: V23 > 0.02s, other >0.03s + >1mm deep
R wave
- Transition: normal V34, early: R>S in V1/2
- Poor R Wave Progression: R <3mm V3
QRS complex
- Duration: 60-110msec normal/ wide; R wave peak time
- Amplitude: normal/ large voltage/ low voltage/ alternans
- Morphology: notched/ RBBB/ LBBB
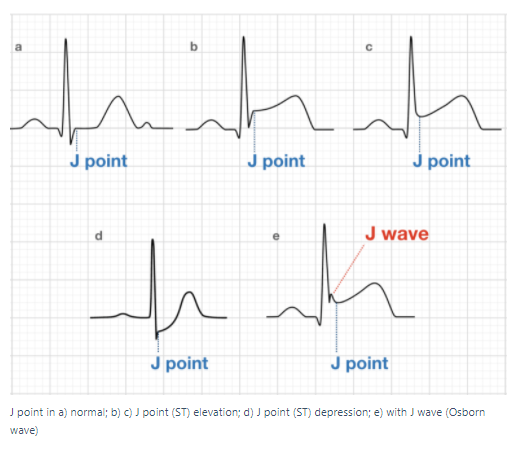
- Displacement: elevation/ depression (J point vs TP interval)
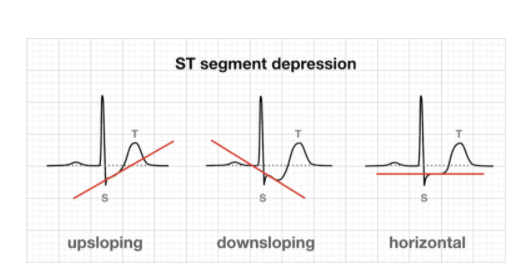
- Contour: horizontal /upsloping / downsloping
T wave
- Amplitude: normal <2/3 R/ peaked/ inversion/ alternans
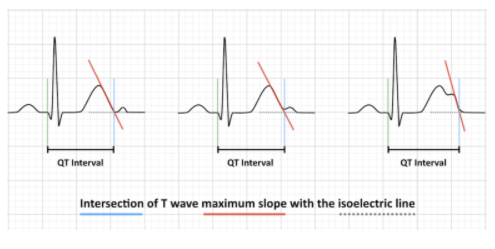
- Duration: normal 390-450 or 460msec / long/ short/ QT dispersion
- Method, 3+ QRS in 3+ leads, QTc formulae, caveats
U wave
- Normal 10% T or <1.5mm/ prominent/ inversion/ alternans
Additional waves
- DOE: Delta wave, Osborn wave, Epsilon Wave
Chamber hypertrophy
Lethal – do not miss!
- Ischaemia – STE criteria and DDX/ Sgarbossa/ reciprocal change/ Wellens/ aVR
- Quick BRAD Walk Home! Lethal causes of syncope:
- Pulmonary Embolus
- Electrolytes: hyperK, hypoK, hypoCa, hyperCa, hypoMg
- Toxicology: TCAs, digoxin
Other tricks and traps
- Dextrocardia, Lead reversals
- Artifacts – tremor artifact
- Pacing spikes – pacemaker malfunction: failure to sense/ capture/ output?
Synthesis
- Leave space to put this at the start of the answer
- Unifying diagnosis, DDx, life threats



