Another great resource on pediatric hypertension is Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Pediatrics. 2017 Sep;140(3):e20171904.
In this post I link to and excerpt from The Cribsiders‘ #36: Off the Cuff – Managing Pediatric Hypertension in Your Primary Care Clinic. OCTOBER 13, 2021 By DR SAM MASUR.
All that follows is from the above resource.
Pediatric Hypertension Pearls
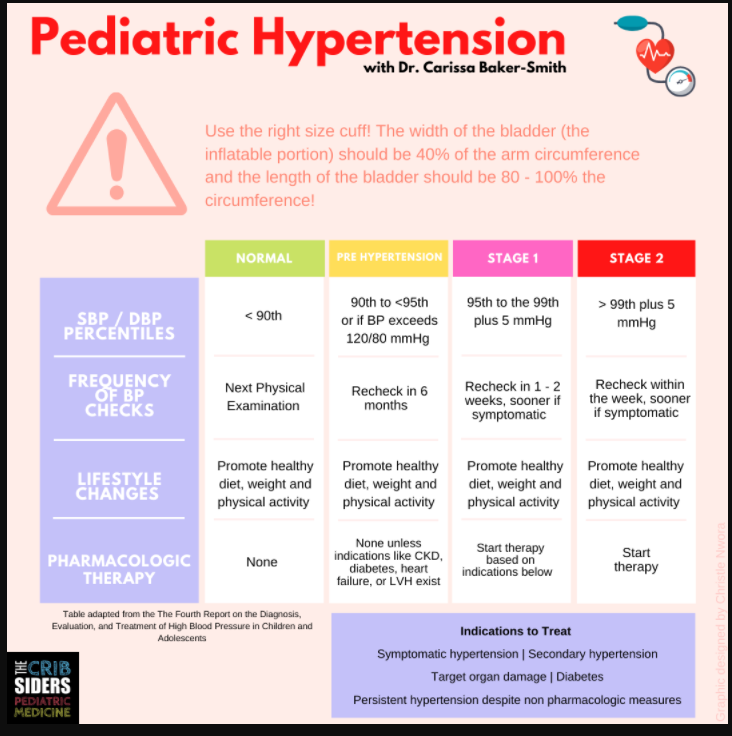
- An appropriate cuff size is a cuff with an inflatable bladder width that is at least 40 percent of the arm circumference and a bladder length that covers 80–100 percent of the circumference of the arms.
- Younger children with elevated blood pressure should raise concern for primary causes of hypertension.*
- Lifestyle modification works best when it fits the context of the child.
*”Children and adolescents ≥6 years of age do not require an extensive evaluation for secondary causes of HTN if they have a positive family history of HTN, are overweight or obese, and/or do not have history or physical examination findings (Table 14) suggestive of a secondary cause of HTN (grade C, moderate recommendation).”
The above is from Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Pediatrics. 2017 Sep;140(3):e20171904.
Defining Pediatric Hypertension
The Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents has a table for pediatric values. Children under the age 13 are classified via percentile.
- under 90% = Normal
- 90-95% or >120/80 (even if this is lower than 90-95%)) = Elevated
- >95% = Hypertension
Children over the age of 13 are classified using adult guidelines.
Elevated blood pressure has some vascular changes and hypertension correlates with target organ damage and long term consequences.