
Medicine Grand Rounds: Navigating Treatment Algorithms in Type 2 Diabetes Mellitus 11/21/17
What follows are slides and excerpts from this Grand Rounds:
[Note to myself the time stamps in the text before each slide refer to the time of first appearance of the slide and can be used then to add text from the corresponding auto transcription.
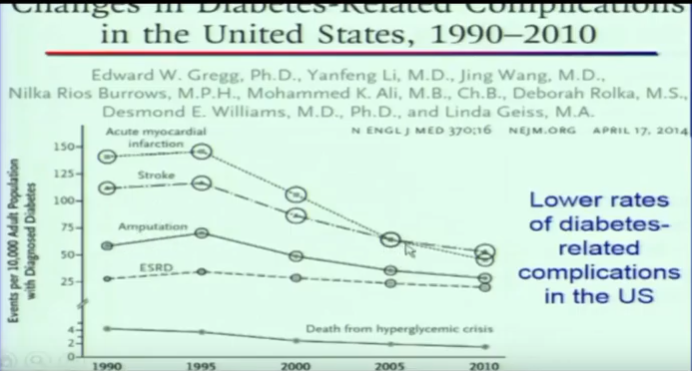
1:28:

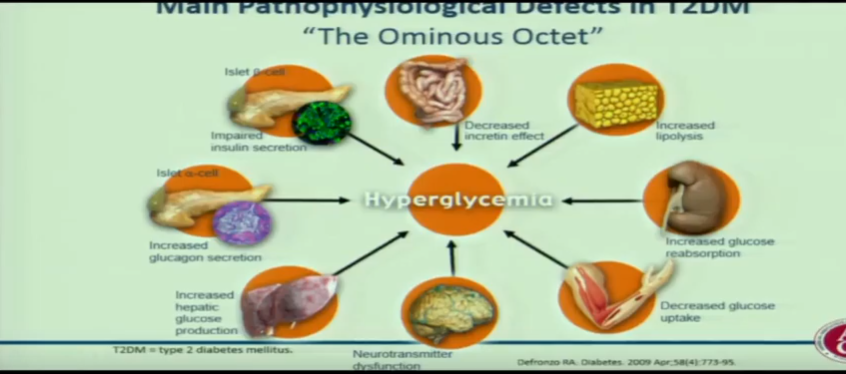
2:42:
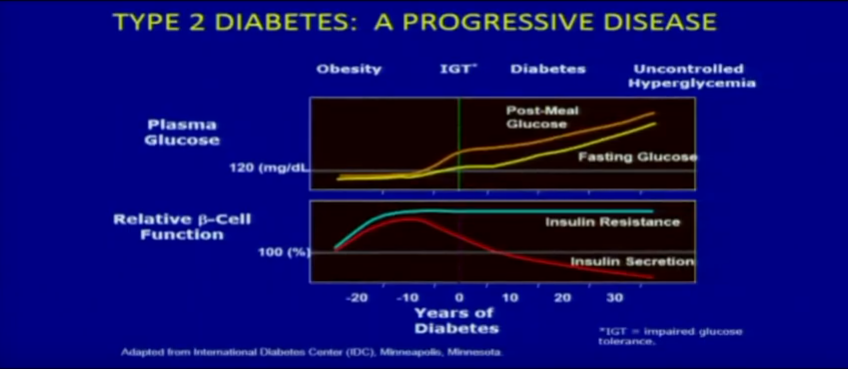
3:03:
3:48:
4:12:
4:36:
4:56

5:38
6:09:
6:41: This summary chart is unreadable and from 2017. So see next slides from 2019 ADA

So instead see Slide 12 below from 2019 ADA Guidelines-Abridged.
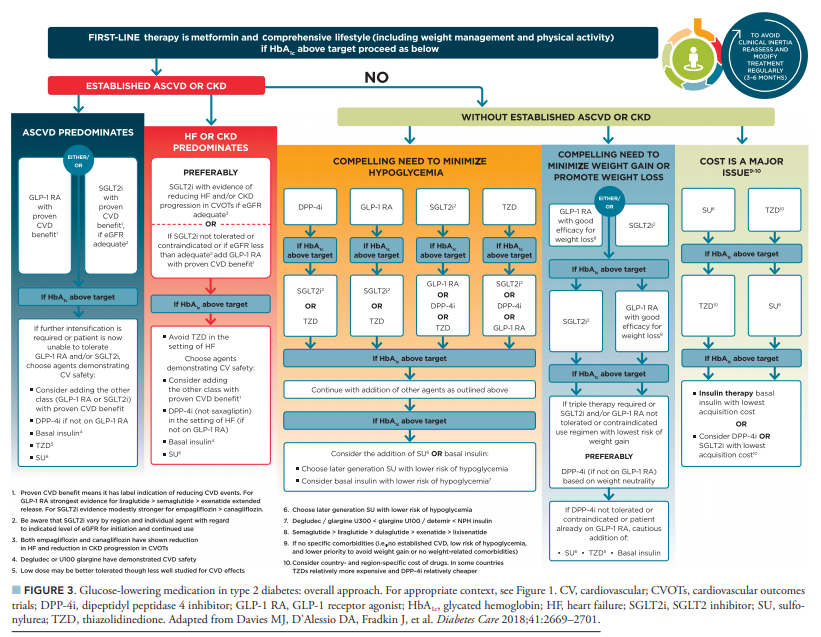
And see also Slide 13 from 2019 ADA Guidelines-Abridged.
7:50: The speaker shows the AACE DM 2017 algorithm. Instead I’ve placed the slide from the 2019 AACE/ACE COMPREHENSIVE TYPE 2 DIABETES
MANAGEMENT ALGORITHM

8:36:
9:36:

9:56

So if someone fails on one medicine [That is the medicine stops working], you don’t switch to another medicine. Rather you add a second medicine to the first medicine [and most of the time the first medicine is metformin].
The combination of different medicines has a dramatic effect because they each have different mechanisms.
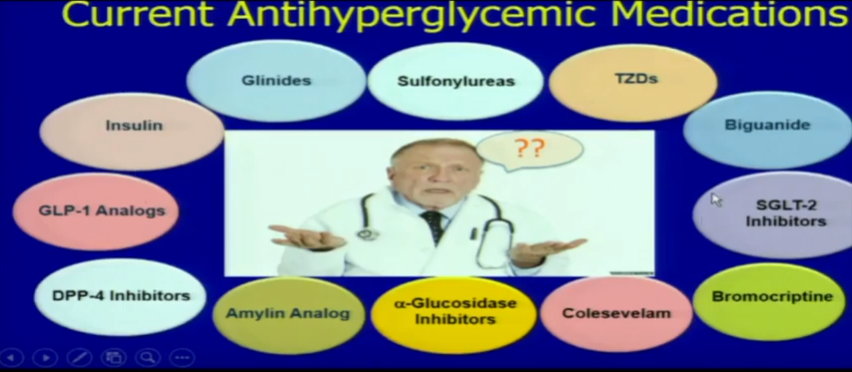
11:45 So the chart below is what the doctors at Emory have come up with as a guide for the second drug after metformin and a list of the names of some of the different medications that we can choose from:
12:30 And here is the list of the names of some of the different kinds of medications we can choose from:
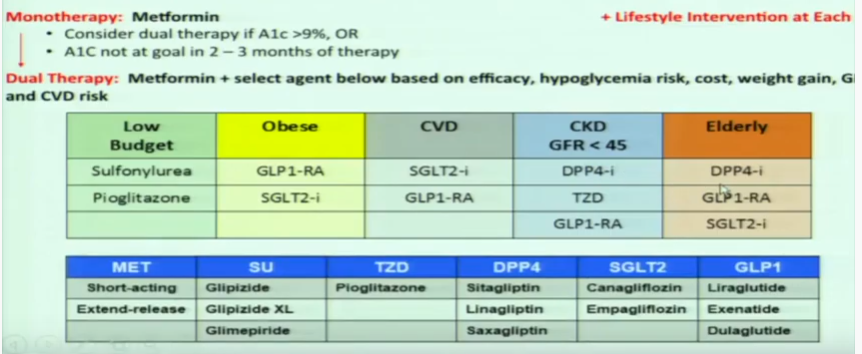
For more information on the drug classes, please see List of Type 2 Diabetes Medication Classes With Links To More Information
Posted on November 6, 2019 by Tom Wade MD
13:10 70% of type 2 diabetics are being started on metformin appropriately. But even in 2016 the most commonly prescribed second medication is sulfonlyurea. The next most common second drug is a DPP4 inhibitor.
The sulfonylureas are only $5 but cause hypoglycemia. DPP4 inhibitors don’t cause hypoglycemia but cost $400.
So we need to make a decision and it has to be individualized.
13:40
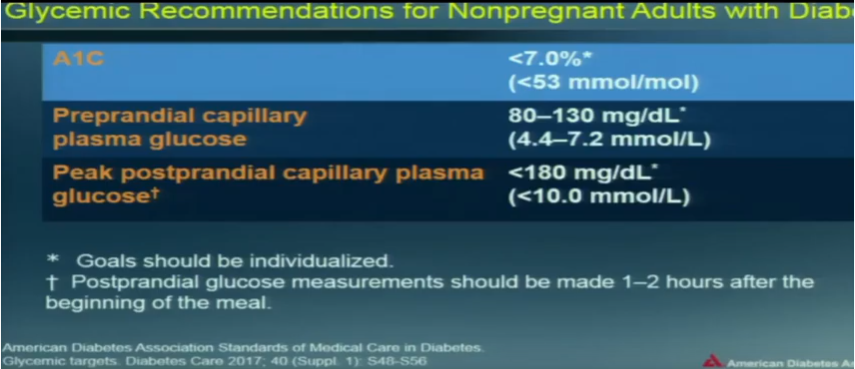
14:25 And in patients we can use the ADA chart below to individualize each patient’s glycemic target.

start at 14:25



