
Dr. Hallberg’s talk, below, is outstanding. The first part of her talk (from the start to 52:30) is the standard basic stuff we need to know to prescribe the ketogenic diet).
For clinicians already well versed in the ketogenic diet, the Question And Answer Period (from 52:30 to the end at 1:13:22) has a great set of answers to common keto diet questions. If you already understand the basics of the ketogenic diet, review this latter part of the talk and also review my advice on implementing the ketogenic diet – interspersed between Dr. Hallberg’s great points.
Here is a link to Ketogenic Diet for Diabetes with Sarah Hallberg, DO. Video is 1:13:32, published September 18, 2018:
Sarah Hallberg, DO: She outlines recent research that suggests patients with metabolic diseases like type 1 and type 2 diabetes can achieve exceptional glycemic control using a low-carb ketogenic diet. Dr. Hallberg also discusses ways to help support patients in the long-term while maintaining this type of diet.
[This Grand Rounds] is from The Institute for Functional Medicine (IFM) in collaboration with Cleveland Clinic Center for Functional Medicine
Here are some slides and excerpts from Dr. Hallberg’s lecture:
49:48
The answer to the slide above is yes. We know that they were following the diet because we measured their beta-hydroxybutyrate levels while they were on the diet. And their beta-hydroxybutyrate levels were elevated.
50:02
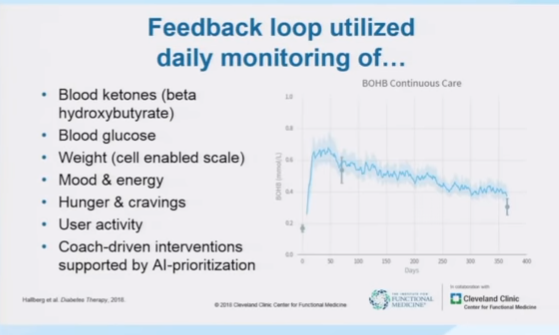
So the above is what Dr. Hallberg’s team monitored to keep the patients encouraged and on track to follow the program.
Although Dr. Hallberg did not mention them, the program undoubtedly has a short online computer form that the patient is asked to complete. And then the health coach and doctor review those forms.
50:19 below
Remember that the program consists of a low carbohydrate diet (less than 30 grams of CHO a day – or better less than 20 grams a day). The patient should have moderate protein intake (1.5 gm of protein per kg of ideal body weight per day). And add fat for the rest of the calories.
Fat is very important because it promotes satiety. No diet is sustainable if the patient is constantly hungry.
The patient won’t be hungry on a well formulated ketogenic diet.
50:45 Most people need long term support to stay with the program.

50:55 And here is how Dr. Hallberg’s program supports the patient so they can stay on the diet program. Each patient recieved:
- A personal health coach with whom they interacted with initially twice a day at the start of the program
- Each patient had a personal physician who monitored their treatment and adjusted their diabetes medicines as their blood sugars improved on the diet
- They had a patient support community where they could share their progress and concerns with other patients in the program [like a private Facebook group]
- Online resources each patient could access [videos, podcasts, and blog posts]
- And an individual online chart where their biomarkers were stored. Thus, the patients could review how they were doing at any time.

At 52:40 Dr. Hallberg answers questions and for me, this was the best of the lecture. It covers many of the subtle points of the ketogenic diet.
The first question is: What about hypokalemia on the ketogenic diet?
52:50 Dr. Hallberg answers:
As long as the patient is taking an adequate amount of sodium, we don’t usually see hypokalemia [and] because we are checking labs all the time.
Dr. Hallberg does follow the potassium levels and again emphasizes the importance of repleating sodium loss. The sodium loss occurs because on a low carbohydrate ketogenic diet the patient will diurese and lose sodium.
Dr. Hallberg states that they put most patients on magnesium supplementation. She states that most U.S. patients whether on a ketogenic diet or not should get magnesium supplementation.
The reason for the above recommendation, Dr. Hallberg states, is because we don’t get magnesium from our fruits and vegetables like we used to because the our soil is now magnesium depleted.
However, for a different view of magnesium, please see “Magnesium Fact Sheet for Health Professionals” From NIH Office Of Dietary Supplements
Posted on November 6, 2019 by Tom Wade MD
54:00: [The question is not heard but is almost certainly: How do we avoid hypoglycemia as the patient’s blood sugars go down as he or she follows the ketogenic diet.]
Here is Dr. Hallberg’s answer:
You have to be on top [of the changing blood sugars].*
*Earlier in her talk, Dr. Hallberg has recommended the Continuous Blood Sugar Monitor as a great way to stay on top of the blood sugars. Here is a link to The First Four Glucose Monitors, July 4, 2018, from Managed Care Magazine. The continous glucose monitor is one of the keys to safely and successfully initiating and following a ketogenic diet.
54:30
Dr. Hallberg states:
[My] expertise is that I am an expert deprescriber.
This [deprescribing] is an art as well as a science.*
*For detailed instruction on deprescribing medications in patients beginning on or continuing on the ketogenic diet, please see Deprescribing Medicines In Type 2 Diabetic Starting And Continuing The Ketogenic Diet
Posted on November 8, 2019 by Tom Wade MD
Now resuming Dr. Hallberg’s lecture:
[We] decrease our patiences’ [diabetic medications even in] . . . the [patients] who have uncontrolled blood sugar when they start [on their ketogenic diet].
[When the patients] start dietary changes [we are following them closely] and oftentimes we are adjusting insulin in some patients on a daily basis.
I remove [the sulfonylurea first] is because it makes patients feel good they can get off [that medicine] either before they start dietary changes or within a week or so [and that is a big win because for them at the beginning of their ketogenic diet program because already you have discontinued one diabetes medicine].
And when do we relax? We relax a little bit when we get them off off the insulin and sulfonylureas.
What follows are my thoughts:
It is also very important to monitor, very frequently at the start, blood pressure, blood pressure medicines, serum sodium, and serum potassium on starting the ketogenic diet because the diet promotes diuresis.
And if the patient is on a diuretic for blood pressure control, you’ll want to decrease or discontinue it if the patient becomes hypotensive, hyponatremic, or hypokalemic.*
*I make the above recommendations because there are numerous medications and medical conditions besides diuretics that can cause hyponatremia (1) and hypokalemia (2).
(1) Hyponatremia in Emergency Medicine Clinical Presentation
Updated: Dec 28, 2018 by Kartik Shah, MD from emedicine.medscape.com
(2) Hypokalemia
Updated: Dec 06, 2018 by Eleanor Lederer, MD, FASN from emedicine.medscape.com
55:27
Resuming Dr. Hallberg’s lecture:
The next thing we go after is the short-acting insulin because if they are eating a well formulated ketogenic diet they shouldn’t need [short acting insulin preprandial meal coverage].
[The] last thing we work on decreasing is long-acting insulin.
55:43:
[The above]being said in some of our patients we will decrease all three of those things before they start dietary changes in some cases
55:51
[And] so it can be challenging [to determine which diabetes medicines to stop because [when the patient] presents to you you don’t really know the degree of insulinopenia that [the patient has].
Dr. Hallberg reminds us that newly diagnosed type 2 diabetics are usually still making a goodly amount of insulin. These patients have a very good chance of getting off insulin completely.
But with time, the type 2 diabetic usually makes less and less insulin.
The above fact is why as the duration of the diabetes increases the patient most often requires additional diabetic medications. At the start of the patient’s disease, metformin may be all that is needed. But over the years as insulin production declines, the patient will need additional medicines added to control blood sugar.
So patients with long standing type 2 diabetes and low endogenous insulin may not be able to totally discontinue insulin.
From 56:00 to the end of the lecture, Dr. Hallberg discusses a number of topics concerning the ketogenic diet.
I found that simply reviewing the YouTube autogenerated transcript is the fastest way to review these points.



