
The following post contains links to and excerpts from the 2017 American Academy of Pediatrics‘ Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents [PubMed Abstract] [Full Text HTML] [Download Full Text PDF]. Pediatrics. 2017 Sep;140(3). pii: e20171904. doi: 10.1542/peds.2017-1904. Epub 2017 Aug 21
Here are some excerpts:
Abstract
These pediatric hypertension guidelines are an update to the 2004 “Fourth Report on the Diagnosis, Evaluation, and Treatment of High Blood Pressure in Children and Adolescents.” Significant changes in these guidelines include (1) the replacement of the term “prehypertension” with the term “elevated blood pressure,” (2) new normative pediatric blood pressure (BP) tables based on normal-weight children, (3) a simplified screening table for identifying BPs needing further evaluation, (4) a simplified BP classification in adolescents ≥13 years of age that aligns with the forthcoming American Heart Association and American College of Cardiology adult BP guidelines, (5) a more limited recommendation to perform screening BP measurements only at preventive care visits, (6) streamlined recommendations on the initial evaluation and management of abnormal BPs, (7) an expanded role for ambulatory BP monitoring in the diagnosis and management of pediatric hypertension, and (8) revised recommendations on when to perform echocardiography in the evaluation of newly diagnosed hypertensive pediatric patients (generally only before medication initiation), along with a revised definition of left ventricular hypertrophy. These guidelines include 30 Key Action Statements and 27 additional recommendations derived from a comprehensive review of almost 15 000 published articles between January 2004 and July 2016. Each Key Action Statement includes level of evidence, benefit-harm relationship, and strength of recommendation. This clinical practice guideline, endorsed by the American Heart Association, is intended to foster a patient- and family-centered approach to care, reduce unnecessary and costly medical interventions, improve patient diagnoses and outcomes, support implementation, and provide direction for future research.

2.1 Prevalence of HTN in Children
Therefore*, the actual prevalence of clinical HTN in children and adolescents is ∼3.5%. 7,8 The prevalence of
persistently elevated BP (formerly termed “prehypertension,” including BP values from the 90th to 94th percentiles or between 120/80 and 130/80 mmHg in adolescents) is also
∼2.2% to 3.5%, with higher rates among children and adolescents who have overweight and obesity. 7,9*”Therefore” refers to earlier cited NHANES data in which the prevalence of pediatric hypertension is higher than reported above and explains the likely cause of the discrepency.
2.2 Awareness, Treatment, and Control of HTN in Children
Of the 32.6% of US adults who have HTN, almost half (17.2%) are not aware they have HTN; even among those who are aware of their condition, only approximately half (54.1%) have controlled BP. 12 Unfortunately, there are no large
studies in which researchers have systematically studied BP awareness or control in youth, although an analysis of prescribing patterns from a nationwide prescription drug
provider found an increase in the number of prescriptions written for high BP in youth from 2004 to 2007. 132.3 Prevalence of HTN Among Children With Various Chronic Conditions
It is well recognized that HTN rates are higher in children with certain chronic conditions, including children with obesity, sleep-disordered breathing (SDB), CKD, and those born preterm. These are described below.
2.3a Children With Obesity
HTN prevalence ranges from 3.8% to 24.8% in youth with overweight and obesity. Rates of HTN increase in a graded fashion with increasing adiposity. 19–24 Similar relationships
are seen between HTN and increasing waist circumference. 4,25,262.3b Children With SDB*
SDB occurs on a spectrum that includes (1) primary snoring, (2) sleep fragmentation, and (3) obstructive sleep apnea syndrome
(OSAS). Researchers in numerous studies have identified an association between SDB and HTN in the pediatric population. 40–42* See the podcast Obstructive Sleep Apnea by Steffany.Charles Nov 28, 2017 from PedsCases.com:
This podcast presents an approach to the management of obstructive sleep apnea (OSA) in children. In this episode, listeners will learn about the pathophysiology of OSA and common causes in the pediatric population, steps to evaluating OSA in a pediatric patient, the role of a PSG in diagnosing OSA, as well as treatment options for OSA. This podcast was developed by Steffany Charles in collaboration with Dr. Joanna MacLean, a pediatric Respirologist and Sleep Specialist at the Stollery Children’s Hospital and the University of Alberta.
Related Content:
Case: Sleep Disorders
2.3c Children With CKD
There are well-established pathophysiologic links between childhood HTN and CKD. Certain forms of CKD can lead to HTN, and untreated HTN can lead to CKD in adults, although evidence for the latter in pediatric patients is lacking. Among children and adolescents with CKD, ∼50% are known to be
hypertensive. 46–48 In children and adolescents with end-stage renal disease (either those on dialysis or after transplant), ∼48% to 79% are hypertensive, with 20% to 70% having uncontrolled HTN. 49–53 Almost 20% of pediatric HTN may be
attributable to CKD. 542.3d Children With History of Prematurity
Abnormal birth history—including preterm birth and low birth weight—has been identified as a risk factor for HTN and other CVD in adults 55; only low birth weight has been associated
with elevated BP in the pediatric age range. 56 One retrospective cohort study showed a prevalence of HTN
of 7.3% among 3 year olds who were born preterm. 572.4 Importance of Diagnosing HTN in Children and Adolescents
Numerous studies have shown that elevated BP in childhood increases the risk for adult HTN and metabolic
syndrome. 10,60–62 Youth with higher BP levels in childhood are also more likely to have persistent HTN as adults. 60,63 . . . Both autopsy 65 and imaging studies 66 have demonstrated
BP-related CV damage in youth. These intermediate markers of CVD (eg, increased LV mass,67 cIMT,68 and pulse wave velocity [PWV]69) are known to predict CV events in adults, making it crucial to diagnose and treat HTN early.Finally, measuring BP at routine well-child visits enables the early detection of primary HTN as well as the detection of asymptomatic HTN secondary to another underlying disorder. Early detection of HTN is vital given the greater relative prevalence of secondary causes of HTN in children compared with adults.
3.1 Definition of HTN (1–18 Years of Age)
Given the lack of outcome data, the current definition of HTN in
children and adolescents is based on the normative distribution of BP in healthy children.1 Because it is a major determinant of BP in growing children, height has been incorporated into the normative data since the publication of the 1996 Working Group Report.1 BP levels should be interpreted on the basis of sex, age, and height to avoid misclassification of children who are either extremely tall or extremely short. It should be noted that the normative data were collected by using an auscultatory technique,1 which may provide different values than measurement obtained by using oscillometric devices or from ABPM.There are still no data to identify a specific level of BP in childhood that leads to adverse CV outcomes
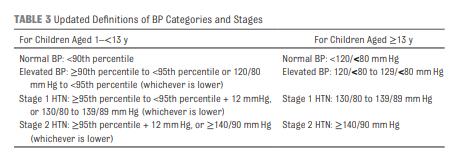
in adulthood. Therefore, the subcommittee decided to maintain a statistical definition for childhood HTN. The staging criteria have been revised for stage 1 and stage 2 HTN for ease of implementation compared with the Fourth Report. For children ≥13 years of age, this staging scheme will seamlessly interface with the 2017 AHA and American College of Cardiology (ACC) adult HTN guideline.* Additionally, the term “prehypertension” has been replaced by the term “elevated blood pressure,” to be consistent with the AHA and ACC guideline and convey the importance of lifestyle measures to prevent the development of HTN (see Table 3).3.2 New BP Tables
New normative BP tables based on normal-weight children are included with these guidelines (see Tables 4 and 5 [on pp 9 – 14 of the PDF). Similar to the tables in the Fourth Report,1 they include SBP and DBP values arranged by age, sex, and height (and height percentile). These values are based on auscultatory measurements obtained from ∼50000 children and adolescents. A new feature in these tables is that the BP values are categorized according to the scheme presented in Table 3 as normal (50th percentile), elevated BP (>90th percentile), stage 1 HTN (≥95th percentile), and stage 2 HTN (≥95th percentile + 12 mmHg). Additionally, actual heights in centimeters and inches are provided.
Unlike the tables in the Fourth Report,1 the BP values in these tables do not include children and adolescents with overweight and obesity (ie, those with a BMI ≥85th percentile); therefore, they represent normative BP values for normal weight youth. The decision to create these new tables was based on evidence of the strong association of both overweight and obesity with elevated BP and HTN. Including patients with overweight and obesity in normative BP tables was thought to create bias. The practical effect of this change is that the BP values in Tables 4 and 5 are several millimeters of mercury lower than in the similar tables in the Fourth Report. 1 These tables are based on the same population data excluding participants with overweight and obesity, and the same methods used
in the Fourth Report.1 The methods and results have been published elsewhere. 77
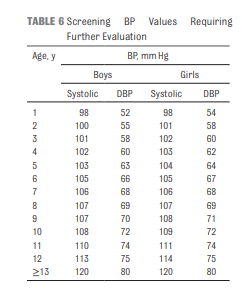
3.2a. Simplified BP Table
This guideline includes a new,
simplified table for initial BP
screening (see Table 6 [above]) based on
the 90th percentile BP for age and
sex for children at the 5th percentile
of height, which gives the values in
the table a negative predictive value
of >99%.
78 This simplified table is
designed as a screening tool only
for the identification of children
and adolescents who need further
evaluation of their BP starting with
repeat BP measurements. It should
not be used to diagnose elevated
BP or HTN by itself. To diagnose
elevated BP or HTN, it is important
to locate the actual cutoffs in the
complete BP tables because the SBP
and DBP cutoffs may be as much as 9
mmHg higher depending on a child’s
age and length or height. A typicaluse case for this simplified table is
for nursing staff to quickly identify
BP that may need further evaluation
by a clinician. For adolescents ≥13
years of age, a threshold of 120/80
mmHg is used in the simplified
table regardless of sex to align with
adult guidelines for the detection of
elevated BP.3.3 Definition of HTN in the Neonate and Infant (0–1 Year of Age)
start here at p 8 of PDF.



