
For further information on subjects related to this post, please see:
Cardiopulmonary Exercise Test: Background, Applicability and Interpretation [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Arq Bras Cardiol. 2016 Nov;107(5):467-481. doi: 10.5935/abc.20160171.
Exercise oximetry step test as part of respiratory assessment and pre-operative assessment in Salford Royal Foundation Trust [Full Text PDF] July 2016. Dr. Ronan R. Driscol.
What follows are excerpts from Pulmonary Hypertension for Primary Care Providers [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Ochsner J. 2009 Winter; 9(4): 234–240:
From The Abstract
Pulmonary hypertension is a constellation of diseases that
shares signs and symptoms of dyspnea, fatigue, chest pain,
palpitations, and syncope. . . . The challenge of the primary care physician is first, identifying pulmonary hypertension, and second, determining the modifiable substrates that contribute to the development and symptoms of this disease.Case Presentation
A 27-year-old woman was referred by her company’s doctor for
syncope. She was told to follow up with a primary care
physician after she passed out at work. She reported that there
was no seizure activity, and she was unconscious for less than a
minute. She remembers waking up and feeling okay. She
described a similar episode when she was in graduate school;
after wearing an electrical heart-recording device for a day, she
was told there was nothing wrong with her. The only other
past medical history she reported is asthma diagnosed in
college. She has had no surgeries, and there is no family history
of disease. Her only prescribed medication is albuterol. She
reported having an old canister that was given to her by
Student Health because she was getting short of breath during
intramural soccer; it never helped her breathing problem. A
review of systems is pertinent for exercise intolerance and dyspnea on exertion, with negative findings for wheezing,
orthostatic dizziness, or any neurologic deficits. Her examinationwas remarkable for a body mass index of 27, oxygen saturation 93%, an accentuated S2, and a holosystolic
murmur at the base that augments with inspiration. No
blood work was performed at this visit. What laboratory
examination would you like to perform? Are there any other
tests you might order?Text
Pulmonary hypertension (PH) is increasingly believed to a play a larger role in a variety of patients’ complaints (ie, dyspnea, fatigue, chest pain, and syncope). The case at the beginning of this article illustrates some of the common presenting signs and symptoms of pulmonary hypertension but also demonstrates some of the pitfalls in diagnosis.
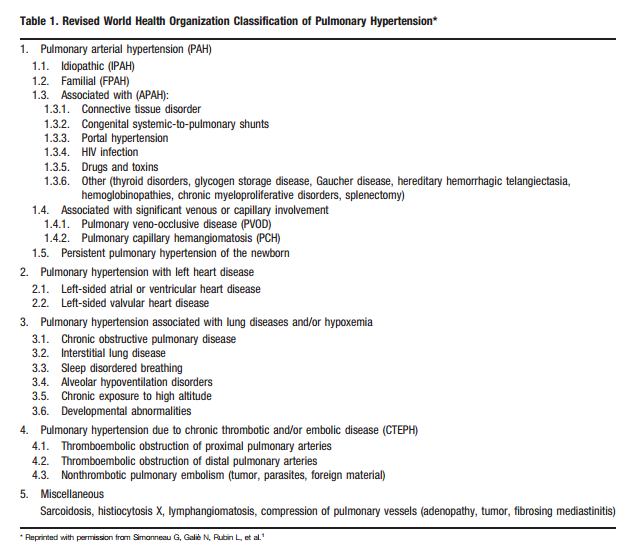
Pulmonary hypertension is best described as a syndrome of dyspnea-related symptoms in the presence of a mean pulmonary arterial pressure of .25 mmHg, regardless of mechanism. Pulmonary hypertensive disorders are classified into groups on the basis of underlying mechanisms, clinical context, and histopathology (Table 1).1


The general practitioner’s primary role in the process of evaluating suspected PH is more commonly oriented toward confirming its presence and identifying associated disease substrate. A PH specialist is oriented toward defining the specific hemodynamic contributions, identifying the underlying cause, determining prognosis, and identifying the most appropriate therapy.
Because of the low prevalence of PH in the general population, global screening is inadvisable. In patients in whom a physician suspects PH, the recommended method of 1-time screening is Doppler echocardiography.17 The frequency of PAH in certain
populations, however, warrants periodic assessment,
and a clinician’s role is to identify through dutiful family
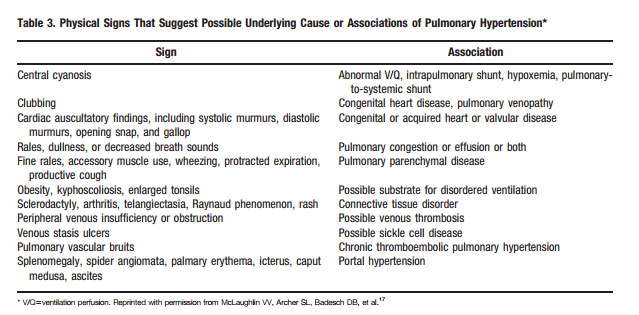
and medical history those patients at risk or with the substrate to warrant assessment. These include patients with family members with known genetic mutations, patients with CTD, or patients with HIV. The optimal frequency of assessment is unclear, but annual assessment is reasonable in these high-risk patients.2In addition to medical and family history, a thorough review of systems and a physical examination should be performed. The aim is to identify and better characterize the common symptoms of dyspnea on exertion, fatigue, chest pain, syncope,
palpitations, or lower extremity edema.As mentioned previously, initial assessment should involve Doppler echocardiography, not only to confirm the presence
of PH but also to assess left heart disease, congenital heart disease, chamber size, function, and valvular heart disease. As dyspnea is a common concern in most patients with PH, obtaining a chest x-ray and pulmonary function testing and polysomnography should be performed to assess for emphysema,fibrosis, thoracic abnormalities, and sleep disorders. If any suspicion of chronic thromboembolism remains, a ventilation perfusion scan or contrast angiography
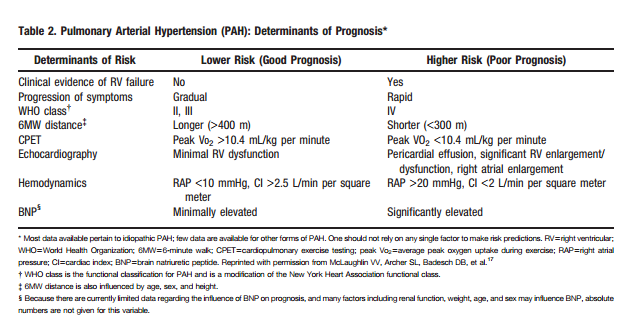
should be performed. The prognostic influences of disease-associated PAH warrant screen laboratory examinations for HIV, CTD, and liver disease. Functionaltesting, right heart catheterization, and vasodilator testing are usually undertaken by a specialist once the diagnosis of PH has been made.



