Today, I review, link to, and excerpt from “Vitamin D for the Prevention of Disease: An Endocrine Society Clinical Practice Guideline”. [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. J Clin Endocrinol Metab. 2024 Jul 12;109(8):1907-1947. doi: 10.1210/clinem/dgae290.
All that follows is from the above resource. Just follow along from the Article Contents below.
Article Contents
Abstract
Numerous studies demonstrate associations between serum concentrations of 25-hydroxyvitamin D (25[OH]D) and a variety of common disorders, including musculoskeletal, metabolic, cardiovascular, malignant, autoimmune, and infectious diseases. Although a causal link between serum 25(OH)D concentrations and many disorders has not been clearly established, these associations have led to widespread supplementation with vitamin D and increased laboratory testing for 25(OH)D in the general population. The benefit-risk ratio of this increase in vitamin D use is not clear, and the optimal vitamin D intake and the role of testing for 25(OH)D for disease prevention remain uncertain.
ObjectiveTo develop clinical guidelines for the use of vitamin D (cholecalciferol [vitamin D3] or ergocalciferol [vitamin D2]) to lower the risk of disease in individuals without established indications for vitamin D treatment or 25(OH)D testing.
MethodsA multidisciplinary panel of clinical experts, along with experts in guideline methodology and systematic literature review, identified and prioritized 14 clinically relevant questions related to the use of vitamin D and 25(OH)D testing to lower the risk of disease. The panel prioritized randomized placebo-controlled trials in general populations (without an established indication for vitamin D treatment or 25[OH]D testing), evaluating the effects of empiric vitamin D administration throughout the lifespan, as well as in select conditions (pregnancy and prediabetes). The panel defined “empiric supplementation” as vitamin D intake that (a) exceeds the Dietary Reference Intakes (DRI) and (b) is implemented without testing for 25(OH)D. Systematic reviews queried electronic databases for publications related to these 14 clinical questions. The Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) methodology was used to assess the certainty of evidence and guide recommendations. The approach incorporated perspectives from a patient representative and considered patient values, costs and resources required, acceptability and feasibility, and impact on health equity of the proposed recommendations. The process to develop this clinical guideline did not use a risk assessment framework and was not designed to replace current DRI for vitamin D.
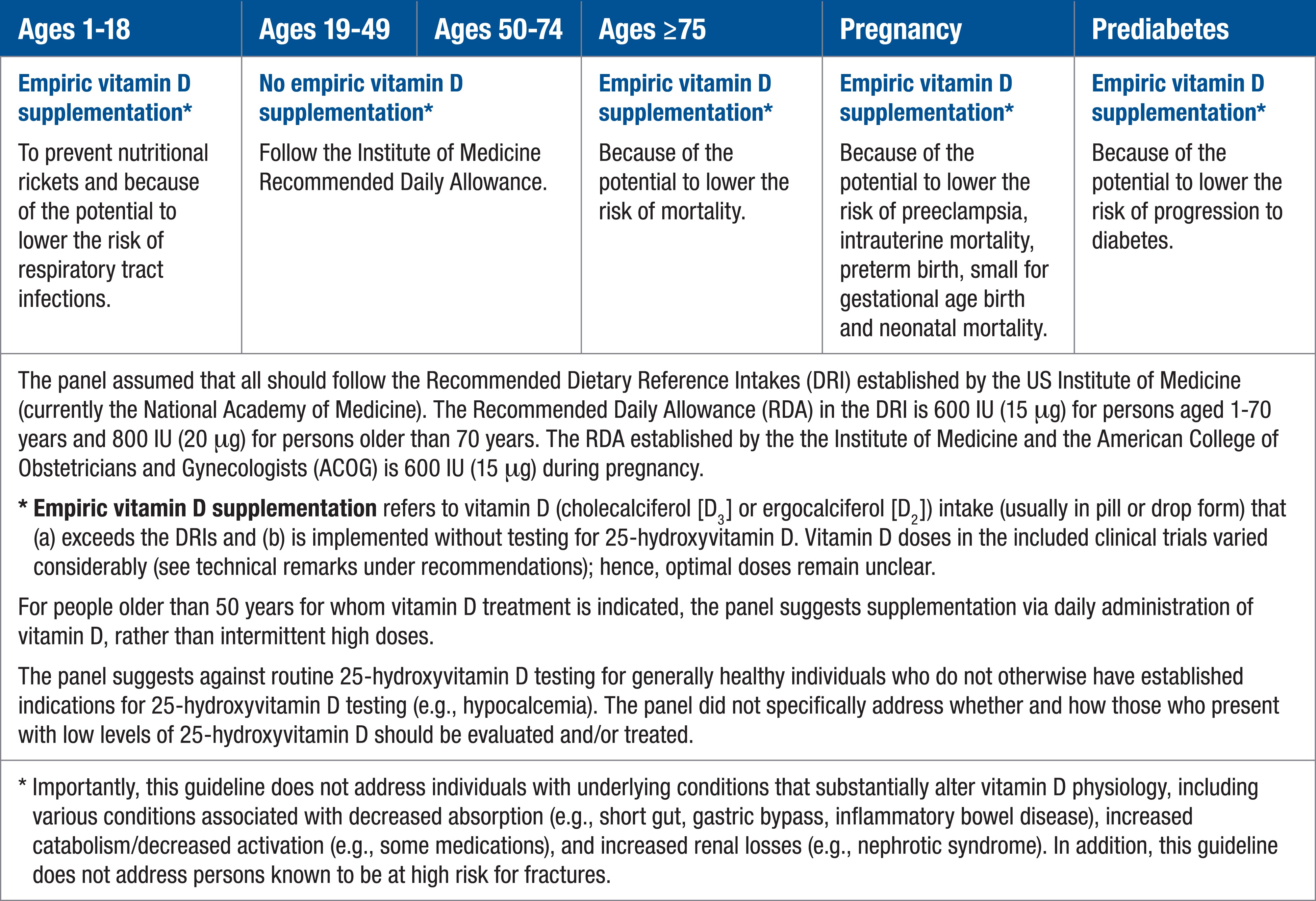
ResultsThe panel suggests empiric vitamin D supplementation for children and adolescents aged 1 to 18 years to prevent nutritional rickets and because of its potential to lower the risk of respiratory tract infections; for those aged 75 years and older because of its potential to lower the risk of mortality; for those who are pregnant because of its potential to lower the risk of preeclampsia, intra-uterine mortality, preterm birth, small-for-gestational-age birth, and neonatal mortality; and for those with high-risk prediabetes because of its potential to reduce progression to diabetes. Because the vitamin D doses in the included clinical trials varied considerably and many trial participants were allowed to continue their own vitamin D–containing supplements, the optimal doses for empiric vitamin D supplementation remain unclear for the populations considered. For nonpregnant people older than 50 years for whom vitamin D is indicated, the panel suggests supplementation via daily administration of vitamin D, rather than intermittent use of high doses. The panel suggests against empiric vitamin D supplementation above the current DRI to lower the risk of disease in healthy adults younger than 75 years. No clinical trial evidence was found to support routine screening for 25(OH)D in the general population, nor in those with obesity or dark complexion, and there was no clear evidence defining the optimal target level of 25(OH)D required for disease prevention in the populations considered; thus, the panel suggests against routine 25(OH)D testing in all populations considered. The panel judged that, in most situations, empiric vitamin D supplementation is inexpensive, feasible, acceptable to both healthy individuals and health care professionals, and has no negative effect on health equity.
ConclusionThe panel suggests empiric vitamin D for those aged 1 to 18 years and adults over 75 years of age, those who are pregnant, and those with high-risk prediabetes. Due to the scarcity of natural food sources rich in vitamin D, empiric supplementation can be achieved through a combination of fortified foods and supplements that contain vitamin D. Based on the absence of supportive clinical trial evidence, the panel suggests against routine 25(OH)D testing in the absence of established indications. These recommendations are not meant to replace the current DRIs for vitamin D, nor do they apply to people with established indications for vitamin D treatment or 25(OH)D testing. Further research is needed to determine optimal 25(OH)D levels for specific health benefits.
Recommendation 12In healthy adults, we suggest against routine screening for 25(OH)D levels. (2 | ⊕◯◯◯)
Technical remarks
In healthy adults, 25(OH)D levels that provide outcome-specific benefits have not been established in clinical trials.
This recommendation relates to adults who do not otherwise have established indications for testing with 25(OH)D levels (eg, hypocalcemia).
Recommendation 13In adults with dark complexion, we suggest against routine screening for 25(OH)D levels. (2 | ⊕◯◯◯)
Technical remarks
This recommendation relates to generally healthy adults with dark complexion who do not otherwise have established indications for 25(OH)D testing (eg, hypocalcemia).
The panel did not identify any clinical trials that related clinical outcomes to skin complexion per se. A secondary analysis did not clearly suggest net benefit with vitamin D in those who self-identify as Black. The panel recognized that self-identified race is an inaccurate and otherwise problematic proxy for dark complexion.
Question 14. Should screening with a 25(OH)D test (with vitamin D supplementation/treatment only if below a threshold) vs no screening with a 25(OH)D test be used for adults with obesity?
Recommendation 14In adults with obesity, we suggest against routine screening for 25(OH)D levels. (2 | ⊕◯◯◯)
Technical remarks
In adults with obesity, 25(OH)D thresholds that provide outcome-specific benefits have not been established in clinical trials.
This recommendation relates to generally healthy adults with obesity who do not otherwise have established indications for 25(OH)D testing (eg, hypocalcemia).
Notes:
The Guideline Development Panel did not find clinical trial evidence that would support establishing distinct 25(OH)D thresholds tied to outcome-specific benefits in the populations examined. Hence, the Endocrine Society no longer endorses the target 25(OH)D level of 30 ng/mL (75 nmol/L) suggested in the previous guideline (15). Similarly, the Endocrine Society no longer endorses specific 25(OH)D levels to define vitamin D sufficiency, insufficiency, and deficiency.
The current guideline suggests against routine 25(OH)D screening (in the absence of well-established indications), including in adults and children with obesity, in adults and children with dark complexion, and during pregnancy. This also represents a change from the 2011 guideline (15).