
After reviewing the HHS report on Joan Rivers endoscopy, I wanted to review the indications for upper GI endoscopy in patients with symptoms of dyspepsia or reflux.
The American Society for Gastrointestinal Endoscopy (ASGE) recommends endoscopy for all patients over the age of 50 yrs who have dyspepsia or reflux symptoms even in the absence of other alarm symptoms.
The British National Institute for Health and Care Excellence (NICE) Resource (5) recommends considering upper GI endoscopy in patients over the age of 55 years with treatment resistant dyspepsia to evaluate for esophageal and stomach cancer. See the resource for other detailed recommendations.
********************************************************************************
What follows are excerpts from this guideline.
The role of endoscopy in dyspepsia [PubMed Abstract] [Full Text PDF]. Gastrointest Endosc. 2015 Aug;82(2):227-32. doi: 10.1016/j.gie.2015.04.003. Epub 2015 May 29.
DEFINITION
Dyspepsia is a poorly characterized syndrome thought to originate from anatomic or functional disorders of the upper GI tract.7-9 Dyspepsia encompasses a variety of symptoms including epigastric discomfort, bloating, anorexia, early satiety, belching or regurgitation, nausea, and heartburn. Rome III criteria define dyspepsia as 1 or more of the following 3 symptoms for 3 months within the initial 6 months of symptom onset10: (1) postprandial fullness, (2) early satiety, and (3) epigastric pain or burning. The symptoms of dyspepsia overlap significantly with those associated with peptic ulcer disease (PUD), GERD, other functional disorders such as epigastric pain syndrome and irritable bowel syndrome, malignancy, adverse effects of medications, pancreatitis, biliary tract disease, vascular disease, and motility disorders. The prevalence of GERD and irritable bowel syndrome is higher in patients with dyspepsia compared with patients without dyspepsia.11,12 Despite the nonspecific nature of symptoms, dyspepsia is associated with poor health-related quality of life and greater psychological distress.13-16
PATIENTS WITH ALARM FEATURES
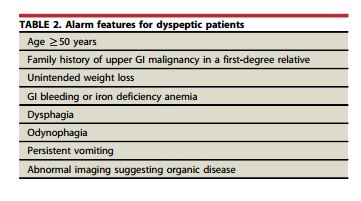
Symptoms of dyspepsia do not reliably identify individuals with malignancy or other important upper GI pathology. Therefore, patient age and alarm features (Table 2) 18 have been used to categorize patients with dyspepsia who may harbor true pathology that may be found with endoscopy or other examinations. Patients with new onset dyspepsia after 45 (18) to 55 (19) years of age (average age 50 years) and those with symptoms or signs that suggest structural disease are advised to undergo initial endoscopy.
Identification of alarm features, however, has a low predictive value for GI cancer. In a meta-analysis of 15 studies evaluating more than 57,000 patients with dyspepsia, alarm symptoms showed a positive predictive value for GI cancer of less than 11% in all but 1 of these studies.20 The negative predictive value of an absence of alarm symptoms was much better at more than 97% due to the low prevalence of GI cancer in this population. A second meta-analysis of 26 studies totaling more than 16,000 patients with dyspepsia similarly showed a positive predictive value and negative predictive value of alarm symptoms for upper GI cancer of 5.9% and greater than 99%, respectively.21 Clinical impression, demographics, risk factors, patient history, and symptoms also do not adequately distinguish structural from functional disease in dyspeptic patients referred for endoscopy.20,22 It is worth noting that one-fourth of patients with malignancy and dyspepsia do not report alarm symptoms.21
In summary, dyspeptic patients older than 50 years of
age or those with alarm features should undergo upper
endoscopy. Endoscopy should be considered for patients
in whom there is a clinical suspicion of malignancy even
in the absence of alarm features.PATIENTS WITHOUT ALARM FEATURES
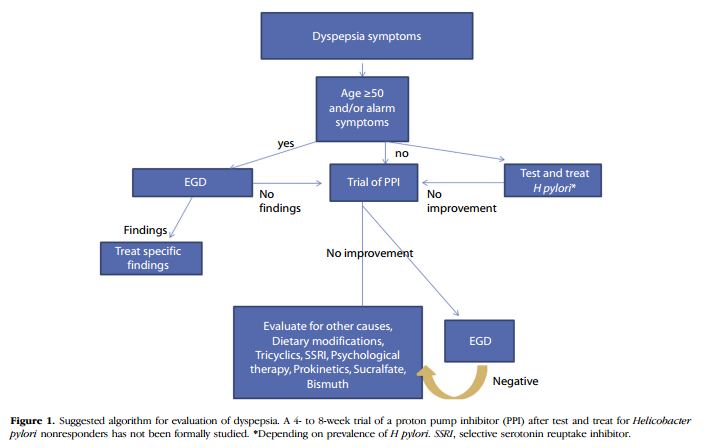
Dyspeptic patients younger than 50 years of age and without alarm features are commonly evaluated by 1 of 3 methods: (1) noninvasive testing for Helicobacter pylori, with subsequent treatment if positive (the “test and treat” approach), (2) an empiric trial of acid suppression, or (3) initial endoscopy.
Endoscopy-negative, persistent dyspepsia
Many patients with dyspepsia and negative findings on endoscopy continue to experience symptoms despite acid suppression and/or H pylori eradication. These patients can be difficult to manage. The majority have functional dyspepsia, for which treatment options include stopping nonsteroidal anti-inflammatory drugs, a trial of antispasmodics, dietary and lifestyle changes, prokinetic agents, sucralfate, simethicone, tricyclic antidepressants, selective serotonin reuptake inhibitors, and cognitive behavior therapy.51,52 More research is required to understand the pathophysiology of symptoms in these patients and the role of medications and other therapies. Other conditions that may cause upper abdominal pain or discomfort (which may be confused with dyspepsia) should be considered, including irritable bowel syndrome, GERD, gastroparesis, pancreatic or biliary disorders, celiac disease, and other functional disorders. Further testing is warranted in patients with pain that is worsening or atypical for dyspepsia or that is accompanied by other worrisome symptoms or signs but should be avoided in young patients with presumed functional disease. A suggested algorithmic approach to dyspepsia is shown in Figure 1.
RECOMMENDATIONS
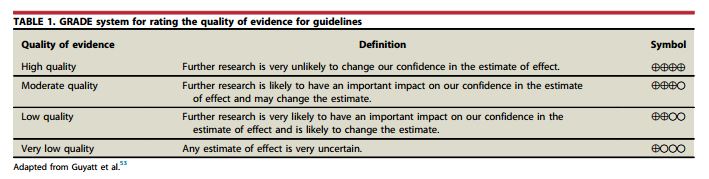
- We recommend initial endoscopy for new-onset dyspepsia in patients 50 years of age of older or those with alarm features.+++0
- We recommend that dyspeptic patients younger than 50 years of age and without alarm features undergo either an initial “test and treat” approach for H pylori or empiric therapy with a PPI, depending on the prevalence of H pylori infection in their population. For H pylori prevalence greater than 20%, “test and treat” is recommended.+++0
- We suggest that dyspeptic patients who are younger than 50 years of age, lack alarm features, and are H pylori negative may be offered a trial of PPI acid suppression.++00
- We suggest that endoscopy be performed in dyspeptic patients who are H pylori negative and do not respond to empiric PPI therapy.++00
Additional Resources:
(1) Diagnostic value of symptoms of oesophagogastric cancers in primary care: a systematic review and meta-analysis [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Br J Gen Pract. 2015 Oct;65(639):e677-91. doi: 10.3399/bjgp15X686941.
(2) Review article: current treatment options and management of functional dyspepsia [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Aliment Pharmacol Ther. 2012 Jul;36(1):3-15. doi: 10.1111/j.1365-2036.2012.05128.x. Epub 2012 May 16.
(3) Meta-analysis: the diagnostic value of alarm symptoms for upper gastrointestinal malignancy [PubMed Abstract] [Full Text HTML]. Aliment Pharmacol Ther. 2004 Nov 15;20(10):1045-52.
(4) Gastro-oesophageal reflux disease and dyspepsia in adults: investigation and management Clinical guideline [CG184] Published date: September 2014 Last updated: November 2014
(5) Suspected cancer: recognition and referral NICE guideline [NG12] Published date: June 2015



