In addition to today’s resources, please review Part 5: Neonatal Resuscitation: 2025 American Heart Association and American Academy of Pediatrics Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Circulation. 2025 Oct 21;152(16_suppl_2):S385-S423. doi: 10.1161/CIR.0000000000001367. Epub 2025 Oct 22.
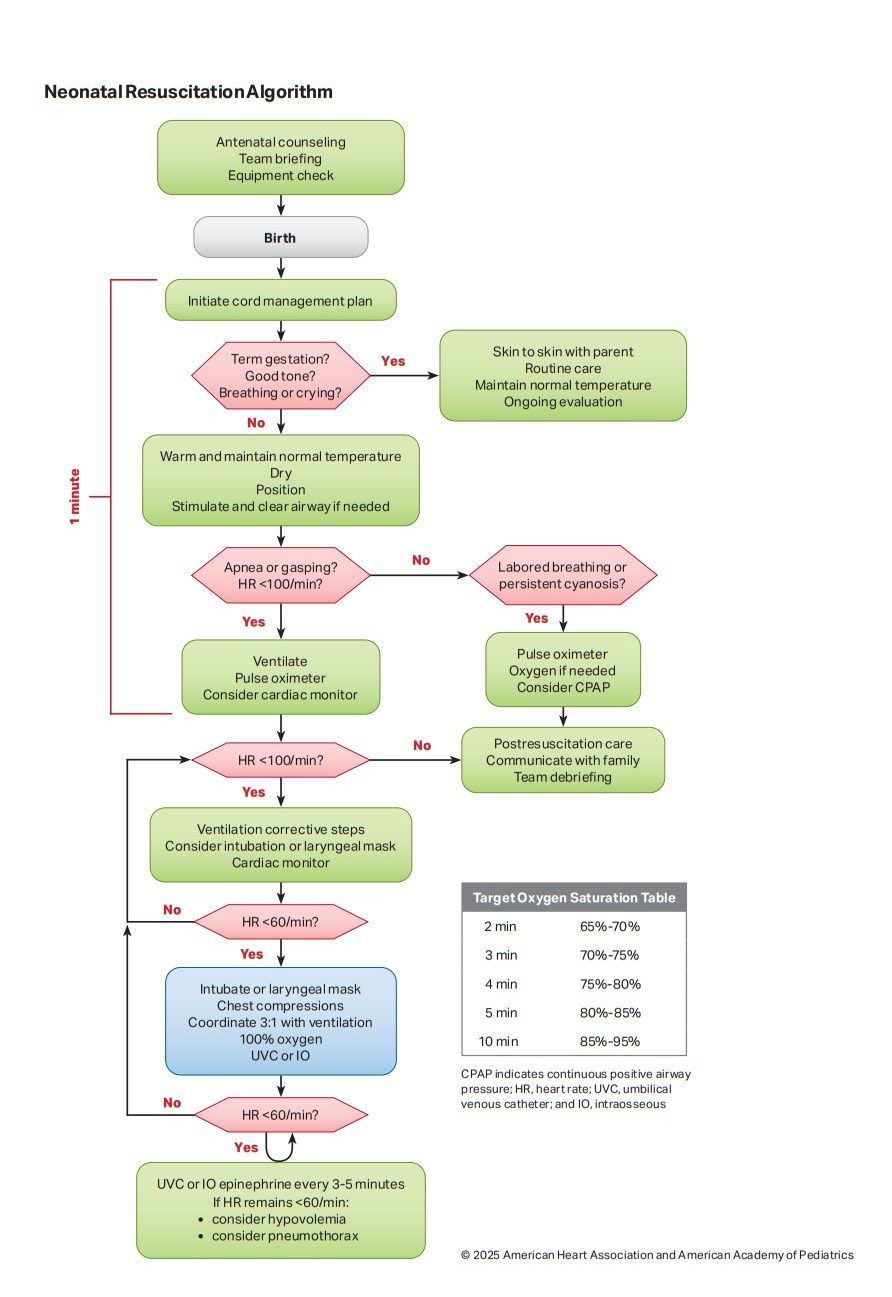
Today, I link to and embed The Neonatal Resuscitation Algorithm along with the Google Search AI overview. All that follows is from the above resources.
The 2025 Neonatal Resuscitation Program (NRP) algorithm prioritizes deferred cord clamping (at least 30–60 seconds), thermoregulation, and immediate, effective Positive Pressure Ventilation (PPV). If the infant has an HR < 100, PPV is initiated. If the HR remains < 60 after 30 seconds of PPV, chest compressions are started. [1, 2, 3, 4, 5]1. Initial Assessment & Routine Care (First 60 Seconds)
- Healthy/Vigorous: If all are present, provide routine care (warm and maintain normal temperature, clear airway if needed, dry, stimulate). Leave infant with the mother. [1, 2]
- Apnea, Gasping, or HR < 100: Proceed immediately to the initial steps: warm and maintain normal temperature, position the airway, clear secretions if needed, dry, and stimulate. [1, 2]
2. Ventilation PhaseAttach a pulse oximeter and consider a cardiac monitor. [1]
- If Apneic/Gasping or HR < 100: Begin PPV within 1 minute of birth. [1]
- Oxygen Strategy: Start with 21% oxygen for infants ≥ 32 weeks gestation, and 30% or higher for infants < 32 weeks. [1]
- Ventilation Rate: 30 to 60 breaths per minute. [1, 2]
- If no improvement/chest not moving: Perform ventilation corrective steps (MR SOPA: Mask adjustment, Reposition airway, Suction mouth/nose, Open mouth, Pressure increase, Alternative airway). [1]
- Reassessment: After 30 seconds of effective PPV, check HR. If HR ≥ 100, slowly discontinue PPV as spontaneous breathing improves. If HR < 60, proceed to chest compressions. [1, 2, 3]
3. Chest CompressionsIf the HR remains < 60 after at least 30 seconds of effective PPV, start chest compressions. [1]
- Ratio & Rate: Use a 3:1 compression-to-ventilation ratio (90 compressions and 30 breaths per minute, total 120 events).
- Oxygen: Increase oxygen to 100%.
- Technique: Two-thumb hands-encircling technique, compressing the sternum to one-third of the anterior-posterior diameter of the chest.
- Airway: Secure the airway (endotracheal tube or laryngeal mask) at this stage.
- Reassessment: Check HR every 30 seconds. [1, 2]