
In addition to the article excerpted below, consider listening to the podcast and reviewing the show notes of #46: Chest pain, coronary CT angiography, and coronary artery disease JULY 3, 2017 By MATTHEW WATTO, MD of The Curbsiders.
The following are excerpts from Resource (1) below [Be sure and visit the article to review all the great picture examples of CT angiography]:
Abstract
The intent of CAD-RADS e Coronary Artery Disease Reporting and Data System is to create a standardized method to communicate findings of coronary CT angiography (coronary CTA) in order to facilitate decision-making regarding further patient management. The suggested CAD-RADS classification is applied on a per-patient basis and represents the highest-grade coronary artery lesion documented by coronary CTA. It ranges from CAD-RADS 0 (Zero) for the complete absence of stenosis and plaque to CAD-RADS 5 for the presence of at least one totally occluded coronary artery and should always be interpreted in conjunction with the impression found in the report. Specific recommendations are provided for further management of patients with stable or acute chest pain based on the CAD-RADS classification. The main goal of CAD-RADS is to standardize reporting of coronary CTA results and to facilitate communication of test results to referring physicians along with suggestions for subsequent patient management. In addition, CAD-RADS will provide a framework of standardization that may benefit education, research, peer-review and quality assurance with the potential to ultimately result in improved quality of care.
1. Introduction
The goal of CAD-RADS, through standardization of report terminology for coronary CTA, is to improve communication between interpreting and referring physicians, facilitate research, and offer mechanisms to contribute to peer review and quality assurance, ultimately resulting in improvements to quality of care. Importantly, CAD-RADS does not substitute the impression section provided by the reading physician and should always be interpreted in conjunction with the more individual and patient-specific information found in the report.
2. Clinical value of coronary CT angiography
Several recent prospective trials have evaluated the clinical utility of coronary CTA and the relevance of CT findings in the context of suspected stable coronary artery disease. They include the PROMISE15 and SCOT-HEART16 trials, which demonstrated that coronary CTA is clinically useful as an alternative to (PROMISE) or in addition to functional testing (SCOT-HEART). Four large randomized trials (CT-STAT, ACRIN-PA, ROMICAT II and CT-COMPARE) compared coronary CTA to the current standard of care in patients with acute chest pain.17e20 Complemented by “real world” implementation data,21,22 they consistently demonstrate the safety of a negative coronary CTA to identify patients for discharge from the emergency department.
3. CAD-RADS reporting system
3.1. CAD-RADS categories
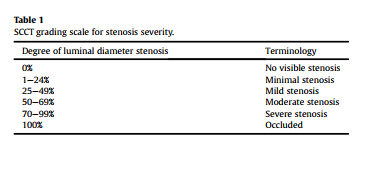
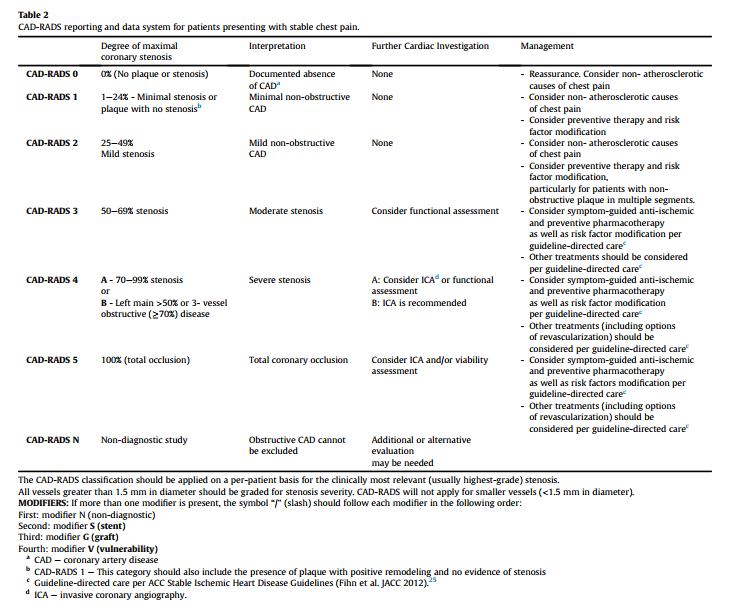
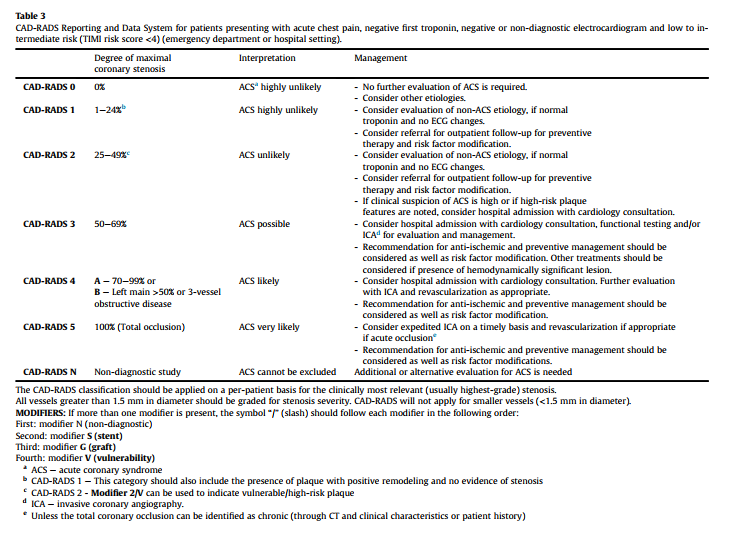
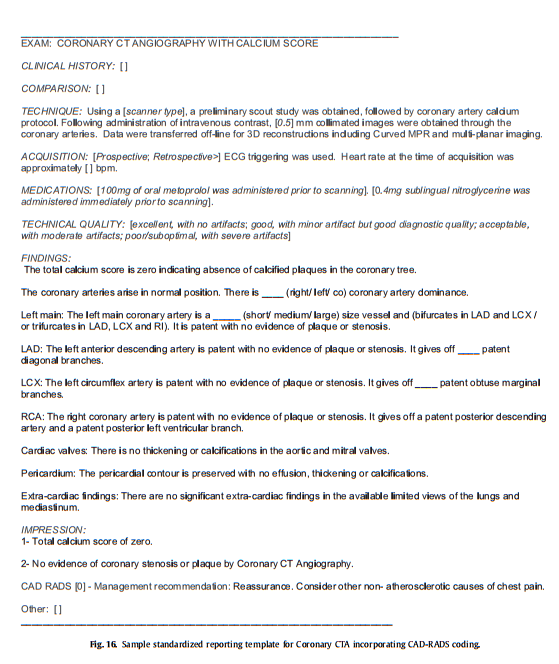
CAD-RADS categories depend on stenosis severity. For the grading of stenosis severity, a classification system suggested by the Society of Cardiovascular Computed Tomography is used (see Table 1). Tables 2 and 3 list the categories of the CAD-RADS reporting system for stable chest pain (Table 2) and acute chest pain (Table 3). They range from CAD-RADS 0 (absence of atherosclerosis) to CAD-RADS 5 (presence of at least one total occlusion) in both settings. Categories should reflect the clinically most relevant finding per patient. Figs. 1e9 provide examples of CAD-RADS categories and sub-categories. It is important to note that CAD-RADS classification is meant to be complementary to the final impression of the report, particularly because the report will provide specific information regarding the location and extent of coronary plaque and stenosis. [Emphasis added. The last figure in this extract is a copy of a sample report.]
3.2. Patients with known CAD
Management recommendations with regard to patients with previously known CAD deserve special consideration. The main clinical benefit of coronary CTA is derived from its high sensitivity and negative predictive value. The positive predictive value of coronary CTA is lower, and especially intermediate lesions may be overestimated regarding their relevance. Many patients with previously known CAD will include lesions that fall into this category, so that coronary CTA will need to be complemented by further tests. Additionally, coronary CTA has low accuracy for diagnosis of in-stent restenosis, particularly in stents smaller than 3.0 mm diameter. Thus, the use of coronary CTA in patients with previously known CAD should be carefully considered. Management decisions derived from coronary CTA results depend on other clinical findings as well as the patient-specific previous history, and should be made on an individual basis.
3.3. Modifiers
CAD-RADS categories can be complemented by modifiers to indicate that a study is not fully evaluable or non-diagnostic (N) or to indicate the presence of stents (S), grafts (G), and vulnerable plaque (V).
3.4. Presence of other cardiac or extra-cardiac findings
Patients undergoing coronary CTA may demonstrate other significant, potentially significant or non-significant cardiac or extracardiac findings. CAD-RADS is intended to focus solely on the classification of coronary artery stenosis and further management. However, other cardiac and extra-cardiac findings of relevance should be reported in coronary CTA studies and should be mentioned in the report text. Specific follow-up and recommendations should be included depending on the pathology.
5. Conclusion
In conclusion, CAD-RADS has been developed based on scientific data, expert guidance from leaders in cardiac imaging and a multi-disciplinary effort involving radiology and cardiology societies (Society of Cardiovascular Computed Tomography, American College of Radiology, American College of Cardiology and North American Society of Cardiac Imaging). It is meant to be an evolving document that will undergo continuous updates as new data are acquired. The main goal of CAD-RADS is to create report standardization terminology for coronary CTA results, and to improve communication of results to referring physicians in a clear and consistent fashion with a final assessment and suggestions for further management. In addition, CAD-RADS will provide a framework to standardize education, research, peer-review, quality assurance and ultimately result in improvement to patient care. Finally, compiling imaging data in a standardized manner will allow to link imaging findings with specific treatments and to better assess the impact on patient outcomes.
Resources
CAD-RADSTM Coronary Artery Disease e Reporting and Data System[PubMed Abstract] [Full Text HTML] [Full Text PDF].
An expert consensus document of the Society of Cardiovascular
Computed Tomography (SCCT), the American College of Radiology
(ACR) and the North American Society for Cardiovascular Imaging
(NASCI). Endorsed by the American College of Cardiology. J Cardiovasc Comput Tomogr. 2016 Jul-Aug;10(4):269-81. doi: 10.1016/j.jcct.2016.04.005. Epub 2016 Jun 15.



