
This summary, Slide 49, contains the critical take home points from this outstanding lecture:
For an outstanding free e-book on neonatology, please see The Iowa Neonatology Handbook:
The Iowa Neonatology Handbook is an ongoing effort by the Division of Neonatology at the University of Iowa Stead Family Children’s Hospital to provide physicians, nurses, and medical students who care for newborn infants a collection of protocols outlining rational approaches to the care of critically ill neonates. This document is not intended to be a comprehensive review of the field of neonatology, nor is it implied that the therapeutic approaches outlined in this book are established policies or standards of care. Rather, they represent a compilation of the experience and clinical styles of the members of our division and are intended only as a guide to therapy.
Here is a link to the outstanding Emergencies In The First Month Of Life From Children’s Hospital Of Philadelphia.
And here is the link to the outstanding clinical pathway ED Pathway for Evaluation/Treatment of Febrile Young Infants (0-56 Days Old) from CHOP.
Here is the link to The Clinical Pathways Library [a comprehensive list of the clinical pathways at Children’s Hospital of Philadelphia (CHOP)].
For a complete list of the outstanding pediatric FOAM courses from the Children’s Hospital of Philadelphia, please see CHOP Open-access Medical Education.
I’ve divided the slides of the lecture into 4 parts.
- Part 1 – Intro and Case 1: Sepsis
- Part 2 – Case 2: Intestinal Catastrophe
- Part 3 – Case 3: Congenital Adrenal Hyperplasia
- Part 4 – Summary and Case 4: Congenital Heart Disease
This post is Part 2: Intestinal Catastrophe.
Slide 1
Slide 3
Slide 18
The above patient’s abdomen is quite distended. He has decreased bowel sounds [and] no palpable masses.
We don’t have any labs yet.
Just based on the history, is there anything else you’d like to know?
Mother was GBS negative and there was no meconium.
An audience member asks another question which the speaker says is a very good question [can’t here the question].
So mother is telling you that he was breast feeding every two to three hours; about ten minutes on each breast; having good wet diapers. He did pass meconium in the first 24 hours.
And on further questioning mom said, “You know, when you asked about the vomitting: It was really green.
So, any concerns there?
Bilious vomitting in a neonate is an intestinal catastrophe until proven otherwise.
Slide 19
Slide 20
The list of neonatal catastrophes is quite extensive but some are more serious than others and associated more with bilious vomitting than others.
But at the top of the list of our differential should be Malrotation With Volvulus because these patients get sick very fast and they can die very quickly in a matter of hours with ischemic bowel perforation.
Slide 21
So let’s talk a little bit about malrotation with volvulus.
Slide 22
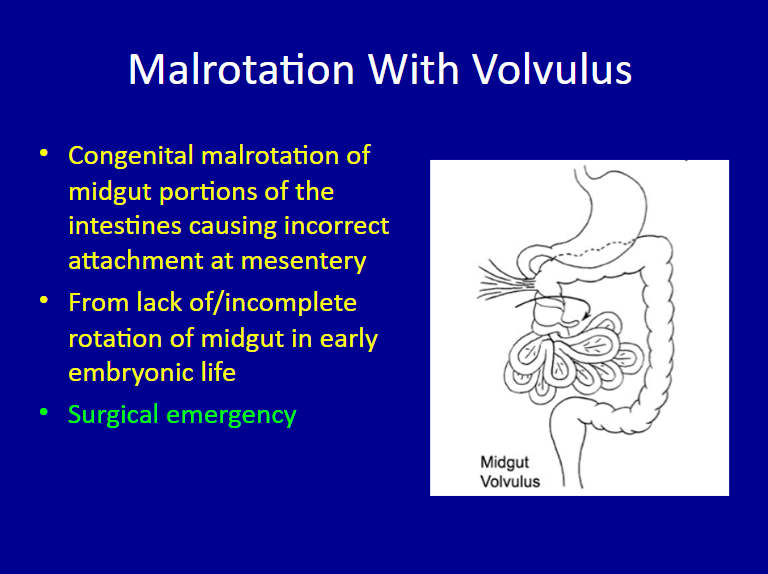
To review what malrotation is:
In malrotation the very narrow pedicle can twist upon itself [and cut off the blood supply]. And if it does that it can cause ischemia and necrosis of the bowel and perforation and these patients can die within a few hours.
Slide 23
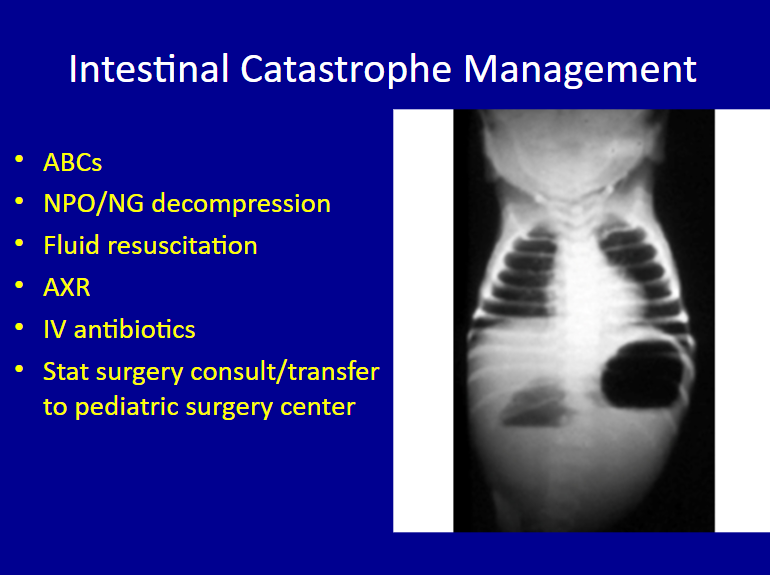
So in a very sick neonate you want to start with your ABCs always. NPO and NG suction, fluid resuscitation, abdominal x-ray and get your pediatric surgeon involved right away or stat transfer to the pediatric surgery center.
This is a very classic presentation [of volvulus] on the [above] x-ray, the double bubble, where you have this distended stomach and small bowel and there is a relatively gas-less abdomen.
But remember, you are not really getting an abdominal x-ray to diagnose malrotation with volvulus.
A lot of times, what we’re really looking for and are concerned about, is free air under the diaphragm to see if there is perforation.
Slide 24
But the diagnostic tool of choice [for the diagnosis of malrotation with midgut volvulus] is the Upper GI [above]. And what you will see is the dye going through the stomach and then sort of the small bowel and coiling around like a corkscrew and it is very abnormal.
Normally,that part of the small bowel should actually be on the left side of the spine.


Here is the link to the third part of the post “Emergencies In The First Month Of Life” – Case 3: Endocrine Emergency – Part 3 Of 4 – Lecture And Slides From CHOP With A Link To Newborn Fever Clinical Pathway



