
So basically the diagnosis of childhood obstructive sleep apnea is with a sleep study when symptoms suggest the diagnosis.
And the treatment of the problem is most often adenotonsillectomy.
And the surgery is commonly performed in non-pediatric hospitals.
Every physician and nurse should have a pre-established plan on how to manage the complications.
And the most feared complication is post-operative bleeding leading to airway compromise or/and exsanguination.
Dr. Sean Fox, of the outstanding Pediatric EM Morsels, has provided us with a clear plan for treating postop tonsillectomy bleeding in Post-Tonsillectomy Hemorrhage. Everyone who might be responsible for this problem should review the post and perhaps consider running an actual team simulation.
So now let’s review the childhood obstructive sleep apnea guideline.
The following is from Resource (1) below.
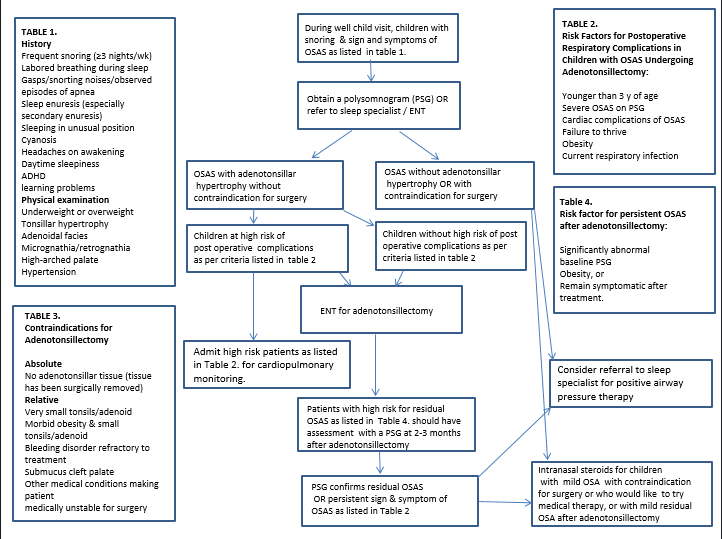
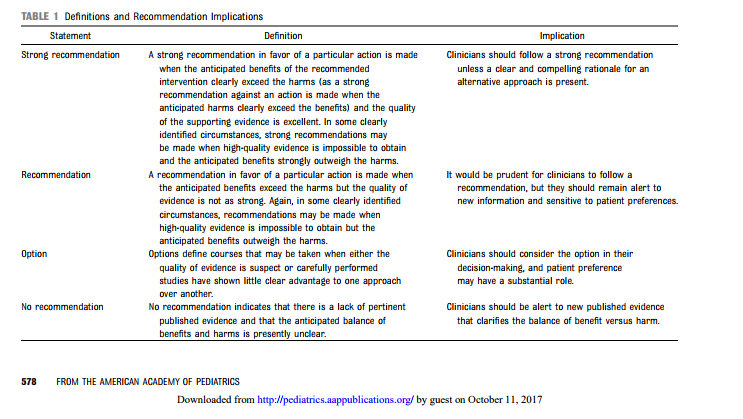
Key Action Statement 2A: Polysomnography
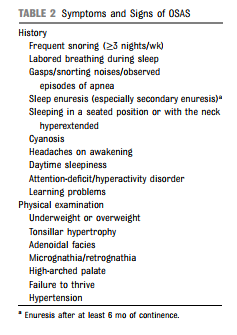
If a child or adolescent snores on a regular basis and has any of the complaints or findings shown in Table 2, clinicians should either (1) obtain a polysomnogram (Evidence Quality A, Key Action strength: Recommendation) OR (2) refer the patient to a sleep specialist or otolaryngologist for a more extensive evaluation (Evidence quality D, Key Action strength: Option). (Evidence Quality: Grade A for polysomnography; Grade D for specialist referral, Recommendation Strength: Recommendation.)
Key Action Statement 2B: Alternative Testing
If polysomnography is not available, then clinicians may order alternative diagnostic tests, such as nocturnal video recording, nocturnal oximetry, daytime nap polysomnography, or ambulatory polysomnography. (Evidence Quality: Grade C,
Recommendation Strength: Option.)Key Action Statement 3: Adenotonsillectomy
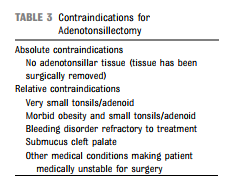
If a child is determined to have OSAS, has a clinical examination consistent with adenotonsillar hypertrophy, and does not have a contraindication to surgery (see Table 3), the clinician should recommend adenotonsillectomy as the first line of treatment. If the child has OSAS but does not have adenotonsillar hypertrophy, other treatment should be considered (see Key Action Statement 6). Clinical judgment is required to determine the benefits of adenotonsillectomy compared with other treatments in obese children with varying degrees of adenotonsillar hypertrophy. (Evidence Quality: Grade B, Recommendation Strength: Recommendation.)
Adenotonsillectomy is very effective in treating OSAS. Adenoidectomy or tonsillectomy alone may not be sufficient, because residual lymphoid tissue may contribute to persistent obstruction. In otherwise healthy children with adenotonsillar hypertrophy, adenotonsillectomy is associated with improvements in symptoms and sequelae of OSAS. Postoperative polysomnography typically shows a major decrease in the number of obstructive events, although some obstructions may still be present. Although obese children may have less satisfactory results, many will be adequately treated with adenotonsillectomy; however, further research is needed to determine which obese children are most likely to benefit from surgery. In this population, the benefits of a 1-time surgical procedure, with a small but real risk of complications, need to be weighed against long-term treatment with CPAP, which is associated with discomfort, disruption of family lifestyle, and risks of poor adherence.
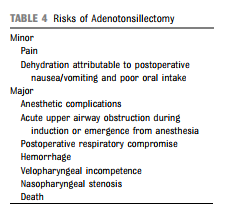
Potential complications of adenotonsillectomy are shown in Table 4 [above]. Although serious complications (including
death) may occur, the rate of these complications is low, and the
risks of complications need to be weighed against the consequences of untreated OSAS. In general, a 1-time only procedure with a relatively low morbidity is preferable to lifelong treatment with CPAP; furthermore, the efficacy of CPAP is limited by generally suboptimal adherence. Other treatment options, such as anti-inflammatory medications, weight loss, or tracheostomy, are less effective, are difficult to achieve, or have higher morbidity, respectively
Key Action Statement 4: High-Risk Patients Undergoing Adenotonsillectomy
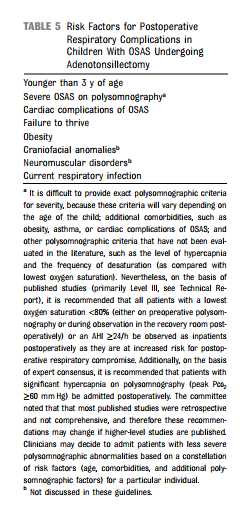
Clinicians should monitor high-risk patients (Table 5) [Above] undergoing adenotonsillectomy as inpatients postoperatively. (Evidence Quality: Grade B, Recommendation Strength: Recommendation.)
Patients with OSAS may develop respiratory complications, such as worsening of OSAS or pulmonary edema, in the immediate postoperative period. Death attributable to respiratory complications in the immediate postoperative period has been reported in patients with severe OSAS. Identified risk factors are shown in Table 5 [Above]. High-risk patients should undergo surgery in a center capable of treating complex pediatric patients. They should be hospitalized overnight for close monitoring postoperatively. Children with an acute respiratory infection on the day of surgery, as documented by fever, cough, and/or wheezing, are at increased risk of postoperative complications and, therefore, should be rescheduled or monitored closely postoperatively. Clinicians should decide on an individual basis whether these patients should be rescheduled, taking into consideration the severity of OSAS in the particular patient and keeping in mind that many children with adenotonsillar hypertrophy have chronic rhinorrhea and nasal congestion, even in the absence of viral infections.
Key Action Statement 5: Reevaluation
Clinicians should clinically reassess all patients with OSAS for persisting signs and symptoms after therapy to determine whether further treatment is required. (Evidence Quality: Grade B, Recommendation Strength: Recommendation.)
Clinicians should reassess OSAS related symptoms and signs (Table 2) after 6 to 8 weeks of therapy to determine whether further evaluation and treatment are indicated. Objective data regarding the timing of the postoperative evaluation are not available. Most clinicians recommend reevaluation 6 to 8 weeks after treatment to allow for healing of the operative site and to allow time for upper airway, cardiac, and central nervous system recovery. Patients who remain symptomatic should undergo objective testing (see Key Action Statement 2) or be referred to a sleep specialist for further evaluation.
Key Action Statement 5B: Reevaluation of High-Risk Patients
Clinicians should reevaluate highrisk patients for persistent OSAS after adenotonsillectomy, includingthose who had a significantly abnormal baseline polysomnogram, have sequelae of OSAS, are obese, or remain symptomatic after treatment,
with an objective test (see Key Action Statement 2) or refer such
patients to a sleep specialist. (Evidence Quality: Grade B, Recommendation Strength: Recommendation.)Numerous studies have shown that a large proportion of children at high risk continue to have some degree of OSAS postoperatively10,13,14; thus, objective evidence is required to determine whether further treatment is necessary.
Key Action Statement 6: CPAP
Clinicians should refer patients for CPAP management if symptoms/ signs (Table 2) or objective evidence of OSAS persists after adenotonsillectomy or if adenotonsillectomy is not performed. (Evidence Quality: Grade B, Recommendation Strength: Recommendation.)
CPAP therapy is delivered by using an electronic device that delivers air at positive pressure via a nasal mask, leading to mechanical stenting of the airway and improved functional residual capacity in the lungs. There is no clear advantage of using bilevel pressure over CPAP.15 CPAP should be managed by an experienced and skilled clinician with expertise in its use in children. CPAP pressure requirements vary among individuals and change over time; thus, CPAP must be titrated in the sleep laboratory before prescribing the device and periodically readjusted thereafter. Behavioral modification therapy may be required, especially for young children or those with developmental delays. Objective monitoring of adherence, by using the equipment software, is important. If adherence is suboptimal, the clinician should institute measures to improve adherence (such as behavioral modification, or treating side effects of CPAP) and institute alternative treatments if these measures are ineffective.
Key Action Statement 7: Weight Loss
Clinicians should recommend weight loss in addition to other therapy if a child/adolescent with OSAS is overweight or obese. (Evidence Quality: Grade C, Recommendation Strength: Recommendation.)
Weight loss has been shown to improve OSAS,16,17 although the degree of weight loss required has not been determined. Because weight loss is a slow and unreliable process, other treatment modalities (such as adenotonsillectomy or CPAP therapy) should be instituted until sufficient weight loss has been achieved and maintained.
Key Action Statement 8: Intranasal Corticosteroids
Clinicians may prescribe topical intranasal corticosteroids for children with mild OSAS in whom adenotonsillectomy is contraindicated or for children with mild postoperative OSAS. (Evidence Quality: Grade B, Recommendation Strength: Option.)
Resources:
(1) Pediatrics. 2012 Sep;130(3):576-84. doi: 10.1542/peds.2012-1671. Epub 2012 Aug 27.
Diagnosis and management of childhood obstructive sleep apnea syndrome [PubMed Abstract] [Full Text HTML] [Full Text PDF].
(2) Post-Tonsillectomy Hemorrhage from Pediatric EM Morsels BY DR SEAN FOX · PUBLISHED AUGUST 17, 2012 · UPDATED JULY 23, 2016. It covers what to do for the patient with massive post op tonsillectomy hemorrhage.
(3) Anesthetic Challenges and Hazards of Pediatric Post Tonsillectomy Hemorrhage from The Department of Anesthesia of The University of Texas Medical School. This is a case of fatal post op tonsillectomy bleeding with a review. Date not available.



