In this post, I link to and excerpt from The Curbsiders‘ #266 Diarrhea Disemboweled Part 1: Acute Diarrhea with Dr. Iris Wang. APRIL 5, 2021 By DR ELENA GIBSON
All that follows is from the above resource.
Transcript-#266-Diarrhea-Disemboweled-Pt.-1-Acute Diarrhea
Flow with us through Diarrhea Disemboweled Part 1 as Dr. Xiao Jing (Iris) Wang @IrisWangMD walks us through the evaluation and management of acute diarrhea.
Acute Diarrhea Pearls
- Diarrhea is “loosely” defined as >3 liquid or loose bowel movements in 24 hours (or more frequently than normal for an individual).
- Diarrhea can be categorized by time as 1) acute <2 weeks 2) persistent 2-4 weeks and 3) chronic >4 weeks.
- Large volume diarrhea is likely a result of pathology located in the small bowel to right colon.
- Diarrhea described as small volume with frequent episodes is likely a result of pathology in the left colon or rectum.
- Red flags for severe acute diarrhea include fever, duration >72hr if immunocompetent (or <72h if immunocompromised), bloody stools, and hypovolemia.
- Broaden the differential for infectious etiologies of acute diarrhea in patients who are immunocompromised to include: cytomegalovirus, Cryptosporidium, Cystoisospora, Mycobacterium avium complex, microsporidia, anddisseminated TB.
- The diagnosis of CMV induced colitis requires endoscopic evaluation and biopsies with pathology-based testing of CMV
- Consider endoscopic evaluation of acute diarrhea in cases of immunosuppression, mycophenolate use, checkpoint inhibitor therapy, or if concern for CMV colitis.
- Treatments for the supportive management of acute diarrhea include oral rehydration solution, loperamide, and bismuth.
C
*2017 Infectious Diseases Society of America Clinical Practice Guidelines for the Diagnosis and Management of Infectious Diarrhea [PubMed Abstract]. Clin Infect Dis. 2017 Nov 29;65(12):e45-e80. Free full text available through the link.
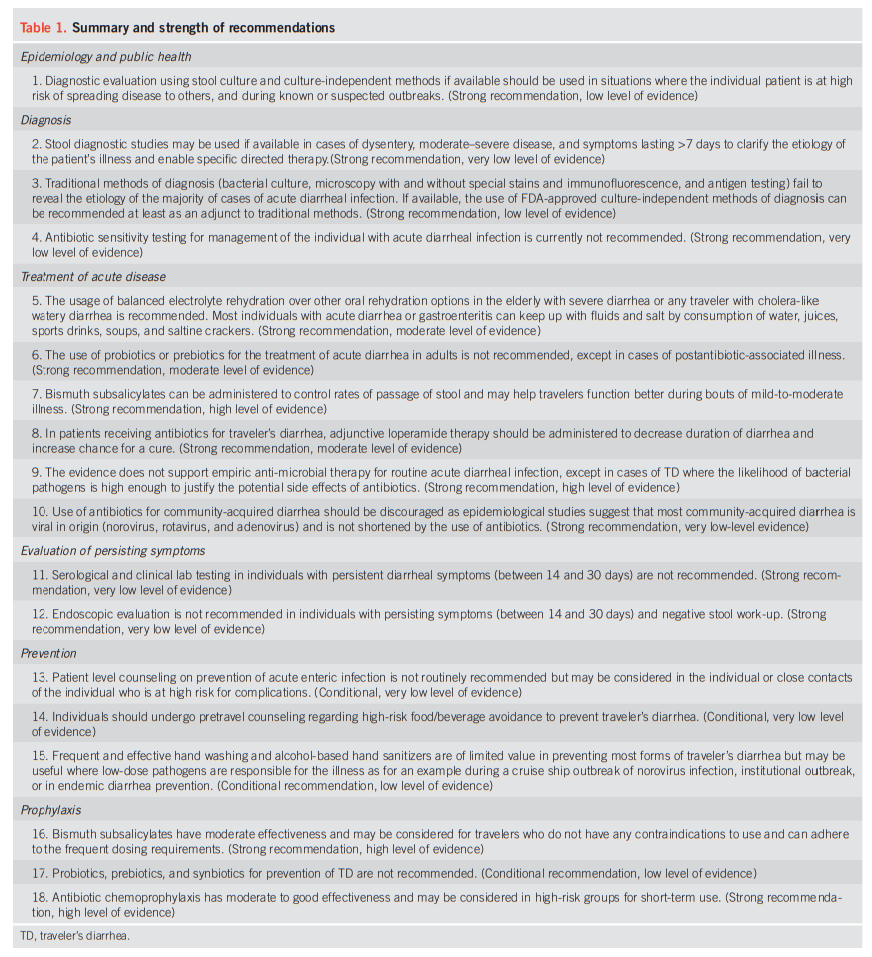
**ACG Clinical Guideline: Diagnosis, Treatment, and Prevention of Acute Diarrheal Infections in Adults [PubMed Abstract]. Am J Gastroenterol. 2016 May;111(5):602-22. Free full text available through the link.
And here are the recommendations from ACG Clinical Guideline above:
Diarrhea: The Initial Evaluation
The History:
It is important to clarify what a patient means by “diarrhea”. Is it loose stools, frequent stools or stool leakage (incontinence issue)? Different people have different baselines for what is normal. Ask about: 1) recent food exposures 2) sick contacts 3) travel or travel of close contacts 4) timeline of symptoms 5) stool characteristics. Understanding if the diarrhea is small volume with increased frequency or less frequent, voluminous diarrhea helps localize the most likely source of pathology. The small bowel is primarily responsible for fluid reabsorption (PO intake and GI tract production) and the large intestine reabsorbs what remains. So, with large volume diarrhea the etiology is likely located from the small bowel to the right colon. The left colon, especially the rectum, serves as a stool reservoir, so pathology there will lead to reduced ability to hold on to stool and increased irritation. Rectal irritation is what causes the sense of needing to pass frequent bowel movements (tenesmus). As a result, frequent bowel movements with small amounts of stool indicate pathology located in the left colon or rectum.
A bit on pathophysiology:
Diarrhea often results from a change in absorption rate that is the result of a change in 1) surface area or 2) contact time. For example, the presence of a large number of unabsorbed osmoles or fat will inhibit water binding for reabsorption and lead to diarrhea.
Red flags:
Fever, Duration (>72 hours in the immunocompetent patient and <72 in immunocompromised patients), bloody stools, signs of hypovolemia (AKI, weakness, dizziness, decreased UOP). Dysentery=grossly blood stools (Riddle 2016). This is important because it is important to differentiate grossly bloody stools from less concerning sources of blood (ie irritation of skin or hemorrhoid from excessive wiping).
Diarrhea: The Lab Evaluation
General Labs:
Check a BMP and CBC to evaluate hydration status, WBC, and Hgb/Hct to evaluate cell counts for infection and anemia.
A microbiologic assessment is recommended in the following cases (Shane 2017):
- Dysentery
- Moderate or severe watery diarrhea
- Increased risk of spreading (ie healthcare worker, food industry worker, daycare worker)
- Prolonged illness (watery and duration >72h)
- Immunosuppression
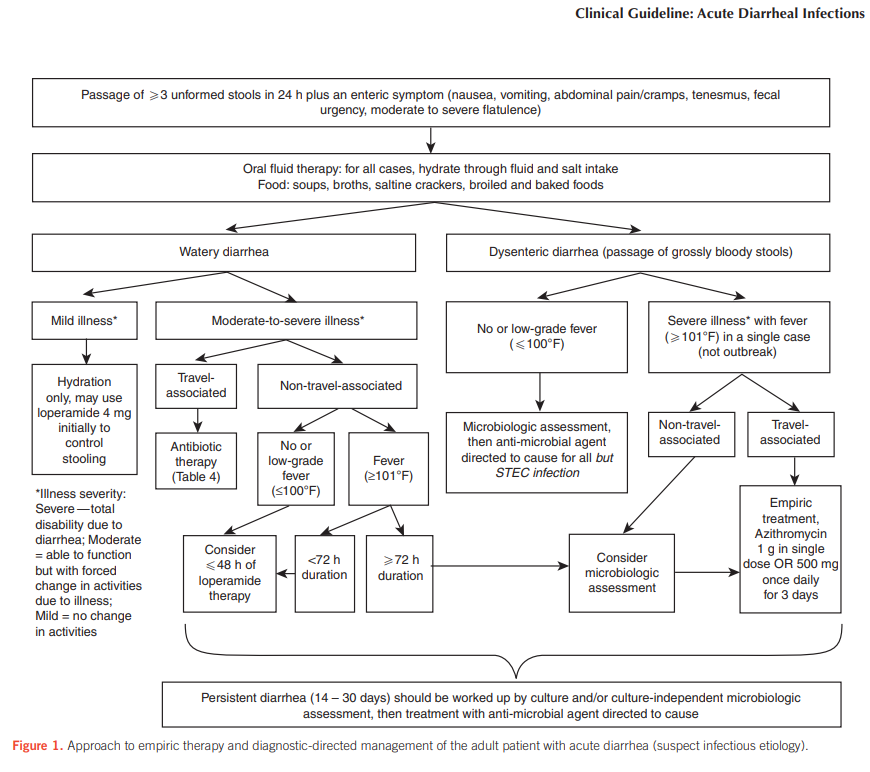
*See ACG guideline flowchart to evaluate this (Riddle 2016; Fig 1) below:
If hospitalization is required, consider early microbiologic assessment for severity. Kashlak Pearl: Dr. Wang recommends considering etiologies of diarrhea that improve with fasting or dietary changes such as osmotic diarrhea if it resolves rapidly following hospital admission.
Microbiological Testing
- Bacterial: There are now various non-culture based panels that test for numerous pathogens (20+) using PCR or antigen testing. These tests are much faster than cultures, but the cost and the risk of “non-pathogenic” positives should be considered (Shane 2017, Hanson 2016). For example, Dr. Wang describes frequently finding positive EPEC results, but these can represent colonization. Regarding cultures, many labs group Salmonella, E Coli, Shigella, Yersenia, and Campylobacter together. If a patient has dysentery, send the PCR panel and cultures for specific organisms known to cause dysentery (EHEC, shigella, entamoeba) —Shane 2017.
- Viral: Testing should be considered in public health reportable cases (ie outbreak in daycare center, cruise ship) and specific cultures and PCR testing needs to be sent (Shane 2017). Don’t forget that COVID19 is one of the acute viral diarrhea pathogens!
Diarrhea Management
Supportive Treatments
For patients with mild illness supportive management = rehydration and loperamide or bismuth (Riddle 2016).
- Loperamide: safe (once C.diff has been ruled out) and effective. Has been associated with toxic megacolon and ileus development in C.diff. See prior Cdiff episode.
- See also Clostridioides (Clostridium) Difficile Colitis. Practice Essentials
Updated: Jul 25, 2019. emedicine.medscape.com- And consider the danger that we all should think about in every diarrhea patient – toxic colitis (toxic megacolon)overview and etiology [Links are to pages of the emedicine.medscape.com article].
- Oral rehydration solution is simple and works in both acute and chronic diarrhea. Sports Drinks (ie Gatorade, Powerade, etc) are not good for rehydration from diarrhea because of 1) the sodium potassium balance; they do not include enough sodium 2) they are hyperosmolar and can worsen diarrhea. Dr. Wang recommends that patients buy something like Pedialyte or make a balanced oral rehydration solution at home. There are recipes online. The ingredients are water with salt and sugar (see instructions from WHO here).
- Bismuth is in the ACG guidelines for consideration for prevention of acute traveler’s diarrhea. Two useful effects of bismuth include 1) antiinflammatory effect of salicylate 2) antimicrobial effect of bismuth. Bismuth subsalicylate does not have the same potential for causing ulcers as other salicylates like aspirin. Caveats: Bismuth requires frequent dosing (3-4x per day), and side effects include: constipation, dark stools and blackening of the tongue.