
In this post, I link to and excerpt from the Curbsiders‘ [Link is to the complete episode list] #296 Diabetes FAQ with Dr. Jeff Colburn, By
All that follows is from the above excellent resource.
Show Segments
- Intro, disclaimer, guest bio
- Guest one-liner, Picks of the Week*
- Case from Kashlak
- Initial Presentation of Diabetes
- Type 1 or Type 2
- Initial Labs, Managing new diagnosis
- Using GLP-1 agonists, SGLT-2 inhibitors
- How to down titrate insulin
- Diabetes in geriatrics
- Diets for diabetes management
- Outro
Sweet, Sweet Diabetes Update Pearls
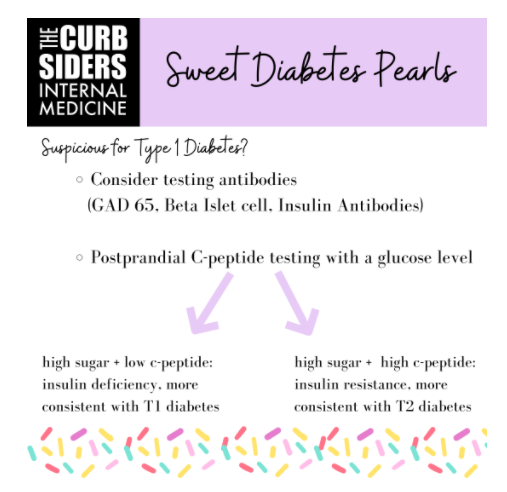
- Age 30 or younger at presentation raises the spectre of T1 diabetes, but you can get T1 at any age. Consider testing for antibodies (GAD 65, Beta Islet cell, Insulin Antibodies).
- BMI alone does NOT indicate Type 1 versus Type 2 Diabetes, per Dr. Colburn.
- Don’t fear GLP-1 agonists and SGLT-2 inhibitors, they are excellent, safe agents for T2DM.
- When trying to down-titrate insulin in the setting of starting one of these new agents, you should aim for a fasting/AM goal glucose of 80 – 130, reducing basal insulin by 2-3 units every 3 days, and monitoring for hypoglycemia, per Dr. Colburn.
- Hypoglycemia is a very real concern, especially for geriatric patients. Hemoglobin A1c target of 8 for geriatric patients may be reasonable.
T1 Versus T2
Age 30 or younger at presentation raises the specter of T1 diabetes, but you can get T1 at any age. Consider testing antibodies (GAD 65, Beta Islet cell, Insulin Antibodies). GAD 65 antibodies are the most sensitive and specific (Towns et al, 2011). However, if antibodies are negative that does not rule out T1 diabetes.
Kashlak Pearl: BMI alone does not indicate T1 vs T2, per Dr. Colburn.
Postprandial C-peptide testing with a glucose level can help differentiate T1 vs. T2. Normal fasting levels c-peptide levels are between 0.3-0.6 nm/L, and prandial levels are between 1-3 nm/L. If the patient has a high blood sugar and low c-peptide: that is insulin deficiency, more consistent with T1 diabetes. If they have a high sugar and a high c-peptide: that is insulin resistance, more consistent with T2 diabetes. But if they are fasting, you may see a normal blood sugar and a normal c-peptide and miss the diagnosis (Leighton 2017).
Data indicate triglycerides may be higher in patients with Type 2 diabetes (Zhao et al, 2019).
Maintain suspicion if a person is failing medical management without insulin that they may indeed have T1, says Dr. Colburn.
Managing a New Diabetes Diagnosis
Severely uncontrolled hyperglycemia can lead to immediate complications like diabetic ketoacidosis (DKA) or polyuria leading to loss of fluid volume and electrolytes.
Refer patients to diabetes education as soon as possible, per Dr. Colburn’s expert opinion. Dietary changes can have profound impact on insulin requirement and hemoglobin A1c. Lowering consumption of carb-heavy liquids and decreasing carb consumption in certain meals (breakfast or lunch) can be an easy first step for patients to tackle. It is also critical to get a sense of what/how they are eating and what their meal structure looks like (ie: some older patients may only be eating one meal a day).
Pre-meal + basal insulin can be overwhelming for patients with new diagnosis of diabetes. Per Dr. Colburn, patients can be started on reasonable basal insulin* dose and metformin, even if we are not sure if they have T1 or T2. Monitoring response to this initial outpatient regimen can help indicate if a patient is insulin resistant versus insulin deficient, as those without any insulin production will fail to get their diabetes under adequate control.
*Basal Insulins (Intermediate and Long Acting) from The Johns Hopkins Patient Guide To Diabetes.
If a patient is very resistant to insulin, you can start with multiple agents. Can follow AACE guidelines or ADA guidelines. Start with metformin, GLP-1 agonist injectables, GLP-1 oral semaglutide (oral and efficacious, Aroda et al, 2019, but expensive), or SGLT-2 inhibitors. The higher sugars are, the more efficacious SGLT-2 inhibitors are (Monami et al, 2013). However, if you are not sure if the patient is insulin deficient, you can induce euglycemic DKA with SGLT-2 Inhibitors. Pathophysiology involves the patient’s sugar normalizing while retaining ketone bodies (Hsia et al, 2017).
Repeat Hgb A1c every three months when adjusting meds or uncontrolled.
Switching Up The Diabetes Regimen
You can do patients a great service by getting them off of sulfonylureas (Dr. Colburn’s expert opinion.) Sulfonylureas can cause hypoglycemia and contribute to weight gain. Both GLP-1 agonists (Filippatos et al, 2014) and SGLT-2 inhibitors (Horii et al, 2020) are good alternatives that do not cause hypoglycemia if they are used as monotherapy, but they can contribute to hypoglycemia in combination with insulin.
GLP-1 agonists: These medicines induce the incretin effect, which impacts many pathways in sugar metabolism (Gilbert et al, 2020). Beneficially, patients lose weight on these agents. Dr. Colburn prefers the 1x week GLP-1 agonists, for efficacy, weight loss, and compliance reasons (Harris et al, 2015). Multiple studies show cardiovascular benefit for high-risk ASCVD patients, particularly for secondary prevention (Sheahan et al, 2020). Dr. Colburn says GLP-1 agonists are labeled as having risk in patients with GFR<30, but most experts would say they are safe and could be used at any GFR and even on dialysis, although some patients may report more nausea. Consider gastric delay issues if patients have severe nausea (expert opinion).
SGLT-2 inhibitors: Another option is an SGLT-2 inhibitor, which causes urinary excretion of sodium, glucose, and water. They are renal protective (Heerspink et al, 2020, Perkovic et al, 2019), although some agents do have GFR cutoffs. Data shows that patients with GFR 15-30 (ie CKD stage 4) do well on SGLT-2 inhibitors, so recommendations about this may change (Chertow 2021). SGLT-2 inhibitors improve CV outcomes (Neal et al, 2017, Hsia et al, 2017).
SGLT-2 inhibitors are associated with increased risk for genital fungal infections (Thong et al,2018) and euglycemic DKA (Hsia et al, 2017).
Ins and Outs of Insulin Taper while starting SGLT-2/GLP-1
When trying to down-titrate insulin in the setting of starting one of these new agents, you should have a fasting/AM goal glucose of 80 – 130, reducing basal insulin by 2-3 units every 3 days, and monitoring for hypoglycemia, per Dr. Colburn.
Expert Opinion: If a patient is on 20 units, can halve to 10 units and go from there with GLP agonist use. If your patient is on a higher basal dose of insulin, like 30-50 units, can do a 20% reduction to ‘make room’ for a GLP 1 agonist. Monitor sugars and make further reductions as needed.
Tricky Diabetes
Take care when managing diabetes in patients who have cognitive decline/dementia. Hypoglycemia is a very real concern given the associated cardiovascular risks, especially for geriatric patients (ADA 2019). A hemoglobin A1c target of 8 for geriatric patients may be reasonable (VA/Dod 2017). Insulin works well in lowering blood sugars, but in geriatric patients the risk of hypoglycemia may be unacceptable. In these populations, Dr. Colburn recommends DDP-4 inhibitors*, especially for a patient who doesn’t need intensive control as these have less hypoglycemic risks. GLP-1 agonists may be an appropriate choice, but Dr. Colburn recommends monitoring for nausea and weight loss in frail patients.
*DPP-IV INHIBITORS from The Johns Hopkins Patient Guide To Diabetes
*Dipeptidyl Peptidase IV (DPP IV) Inhibitors, Srinivasa Venkata Siva Kumar Kasina; Krishna M. Baradhi. Last Update: July 26, 2021, from StatPearls.
Diet-betes?
Diabetes can improve substantially with diet (Lean et al, 2018) but requires motivation and adherence. If patients are on higher dose insulin, (more than 20U) they’re probably insulin deficient and may not be able to do this, per Dr. Colburn. Ketogenic diets cause weight loss but it can be hard to maintain and the lipid profile looks horrendous, says Dr. Colburn. Dr. Colburn says intermittent fasting may be worth a shot in the right, healthy, young patient.



