
In this post I link to and excerpt from EMCrit 115 – A New Paradigm for Post-Intubation Pain, Agitation, and Delirium (PAD). [Link is to the podcast and show notes]. January 13, 2014 by Dr Scott Weingart
This EMCrit 115 is part of Dr Weingart’s minicourse [my term] EMCrit – Critical Care for Non-Intensivists during COVID19 Pandemic [Link is to his excellent post-I’m working my way through all of his resources on the post].
March 25, 2020 by Dr Scott Weingart
Here is the podcast of EMCrit 115:
Dr. Weingart reminds us that excellent management of patients on ventilators requires effective analgesia as well as sedation.
Having an ET tube in your mouth and trachea is a painful miserable sensation. The patient needs pain medicine. If you don’t do appropriate pain control you will have to way over sedate the patient and maybe even paralyze him/her.
And here are excerpts from the show notes:
A1 Sedation [Means] Analgesia First
Stick your finger down your throat–now leave it there.
[You are miserable and that is how an ET tube feels in a patient. So Analgesia first and then sedation.]
Analgosedation: A Paradigm Shift in Intensive Care Unit Sedation Practice [PubMed Abstract] [Full Text PDF]. Ann Pharmacother. 2012 Apr;46(4):530-40.
Just put patients on a fentanyl drip. If not go with dilaudad IV. When remifentanil is cheap, we’ll switch to that in a bunch of patient categories.[cite]15329588[/cite]
Then evaluate pain and decide if the patient needs additional pushes of pain meds.
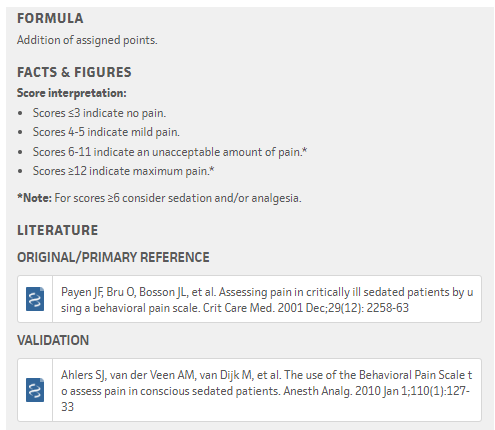
Consider using the Behavioral Pain Scale (Crit Care Med 2001;29(12):2258) HT to Nikolay Yusupov
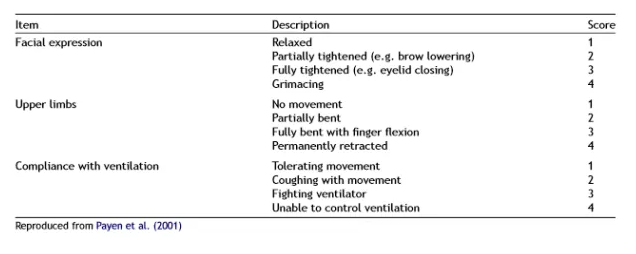
To score the Behavioral Pain Score [from MDCalc – Behavioral Pain Scale (BPS) for Pain Assessment in Intubated Patients: Quantifies pain in intubated patients.]:
Myth – Short-Acting Sedatives and Analgesics Go Away Quickly
You need a goal, like RASSHere is the RASS Scale from the amazing ICU Delirium Site



