
In addition to the resource in this post, please see also Links To And Excerpts From The Curbsiders’ #254 Hypertension Update With Additional Resources On Primary Aldosteronism
Posted on February 5, 2021 by Tom Wade MD
In this post I link to and excerpt from the Kaiser Permanente February 2019 Clinical Practice Guideline on Hypertension.
Here are excerpts:
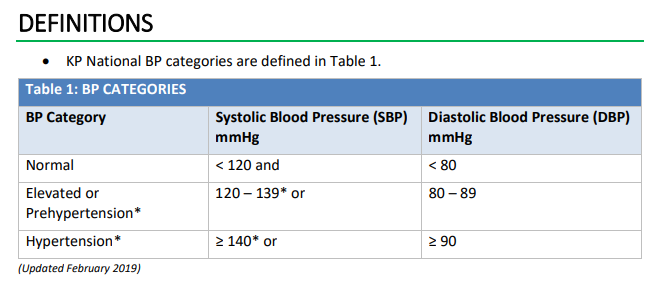
• *Hypertension may also be diagnosed in adults with SBP 130-139, when starting or
taking a blood pressure medicine, and with at least one of the following: ASCVD, CKD,
age ≥ 75 years, or 10-year ASCVD risk** ≥ 10%.
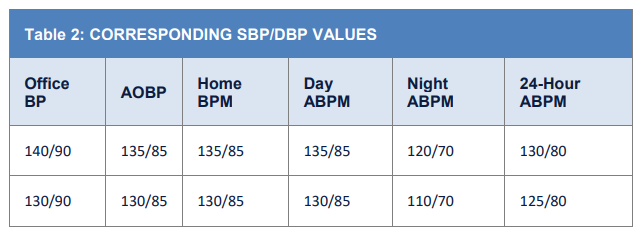
• BP values in this table and elsewhere in this document refer to standard office BP
measurements unless otherwise specified. See Table 2 for corresponding SBP/DBP
values.
• ASCVD, atherosclerotic cardiovascular disease. CKD, chronic kidney disease.
• 10-year ASCVD risk** is the risk of fatal or nonfatal myocardial infarctions or strokes in
adults.**A region may choose which tool (and corresponding cut-point) to use for calculating 10-year ASCVD risk
based on regional needs. Kaiser Permanente ASCVD Risk Estimator (KPARE)* of 10% correlates approximately
with ACC/AHA ASCVD Risk [Calculator]** of 15% and Framingham Risk Score of 15% (used in SPRINT) at the population level.
*Please see the following:
- Abstract 12623: A New ASCVD Risk Estimator is More Accurate Than the ACC/AHA Pooled Cohort Equation in Four Diverse Community-Based Populations in the U.S. and Canada. Originally published5 Nov 2018Circulation. 2018;138:A12623
- “The Kaiser Permanente ASCVD Risk Estimator (KPARE) was developed to address the systematic overestimation of actual ASCVD risk by the ACC/AHA ASCVD Pooled Cohort Equation (ACC/AHA PCE) in contemporary populations.”
- I was unable to locate an online link to The Kaiser Permanente ASCVD Risk Estimator (KPARE)
**Please see the following:
- ACC/AHA CV Risk Calculator (2013) from Medscape.
Returning now to excerpts from the Kaiser Permanente February 2019 Clinical Practice Guideline on Hypertension:
SCREENING
Screening and Diagnosis of High Blood Pressure
- Screen adults aged ≥ 18 years for high BP.
- In adults aged 18-39 years with BP < 130/85 mmHg without other risk factors, screen every 3 to 5 years.
- In adults aged ≥ 40 years and those at increased risk of high BP, screen annually.
Adults at increased risk include those who have BP ≥ 130/85 mmHg or are overweight, obese, or Black/African American.- Obtain measurements outside of the clinical setting for diagnostic confirmation before starting treatment.
- BP readings equal to or higher than those in Table 2, Row 1 confirms the diagnosis of hypertension. Use clinical judgment or regional protocol if obtaining BP outside the clinical setting is not possible. Automated office blood pressure (AOBP) measurements
at ≥ 2 visits may be used.- Diagnose hypertension for BP ≥ 180/110 at a single office reading or ≥ 150/100 with clinical evidence of target organ damage (left ventricular hypertrophy, hypertensive retinopathy, or hypertensive nephropathy).
Office BP: Taken in the clinic setting using an oscillometric (preferred) or aneroid device but not including automated office BP.
AOBP: Taken in the clinic setting using a commercially available device that allows for measurements to be taken with patient unobserved.
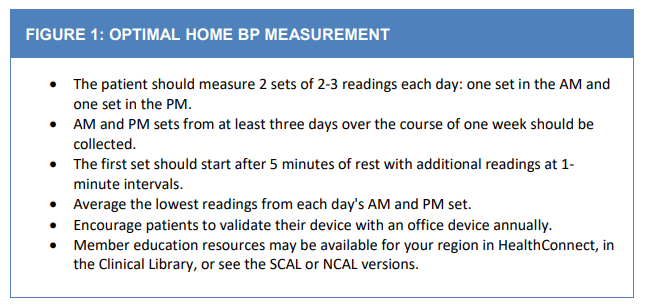
Home BP Monitoring (Home BPM): Taken by the patient at home (see Box 1).
Ambulatory BP Monitoring (ABPM): Taken at regular intervals by a device worn by the patient, usually for 24 hours.
TREATMENT INITIATION, BLOOD PRESSURE TARGETS, AND TYPICAL TESTS
ALL ADULTS
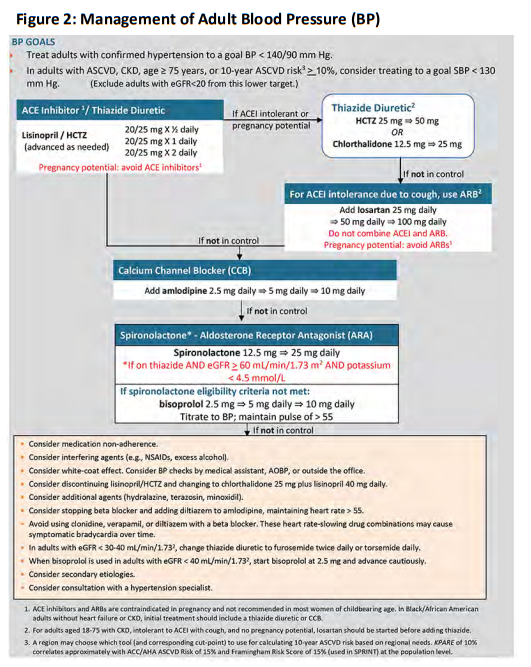
• In adults with confirmed hypertension, initiate pharmacologic treatment to lower BP at
SBP ≥ 140mmHg or DBP ≥ 90 mmHg and treat to a goal SBP < 140 mmHg and goal DBP < 90 mmHg (Table 2, Row 1).SBP < 130 mmHg
• In adults with ASCVD, CKD, age ≥ 75 years, or 10-year ASCVD risk** ≥ 10%, consider pharmacologic treatment at SBP ≥ 130 mmHg and treat to a goal SBP of < 130 mmHg (Table 2, Row 2). Incorporate BP monitoring details, medication benefits and risks, and patient preferences when deciding whether to treat to this lower target.
Exclude adults with eGFR < 20 mL/min/1.732 from this lower target.
**A region may choose which tool (and corresponding cut-point) to use for calculating 10-year ASCVD risk based on regional needs. KPARE of 10% correlates approximately with ACC/AHA ASCVD Risk of 15% and Framingham Risk Score of 15% (used in SPRINT) at the population level.
DM
• DM alone does not qualify for goal SBP < 130 mmHg. DM is a variable in KPARE.
ELDERLY OR FRAIL ADULTS
• Because elderly or frail adults are at higher risk for postural hypotension, check standing BP to guide treatment decisions.
• Incorporate BP monitoring details, medication benefits and risks, and patient preferences in elderly or frail adultsDOWN-TITRATION
• Consider down-titration of BP medication in adults with SBP < 110 mmHg without other indications for medication, such as heart failure, or with symptoms of orthostasis.
TYPICAL TESTS
• Typical tests for adults with a new diagnosis of hypertension may include: fasting glucose or hemoglobin A1C, lipid panel, creatinine with eGFR, sodium, potassium,
calcium, thyroid stimulating hormone, complete blood count, urinalysis, and electrocardiogram.PHARMACOTHERAPY AND MONITORING
ATTAIN AND MAINTAIN GOAL BP
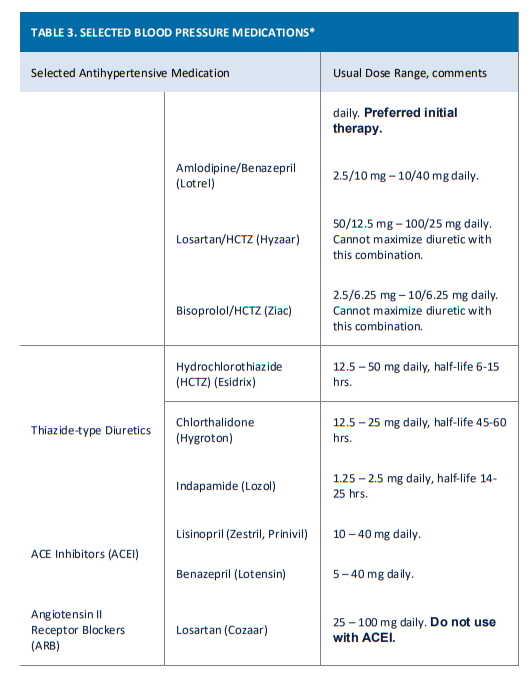
- The main objective of BP treatment is to attain and maintain goal BP. If goal BP is not reached within a month of treatment, consider increasing the dose of the initial drug or add a second drug from one of the thiazide-type diuretic, angiotensin-converting
enzyme inhibitor (ACEI), angiotensin receptor blocker (ARB), or calcium channel blocker (CCB) classes. The clinician should consider continued assessment of BP and adjustment of the treatment regimen until goal BP is reached. If goal BP cannot be reached with 2 drugs, consider adding and titrating a third drug from the indicated classes. If goal BP cannot be reached using only the drugs in these classes because of contraindications or the need for > 3 drugs to reach goal BP, antihypertensive drugs from other classes can
be considered. Consider referral to a hypertension specialist for patients in whom goal BP cannot be attained using the above strategy or for the management of complicated patients for whom additional clinical consultation is needed.DRUG-DRUG INTERACTION
• Simultaneous use of an ACEI, ARB, and/or renin inhibitor is potentially harmful and is not recommended.
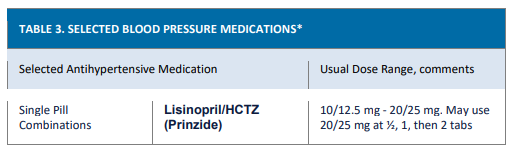
INITIAL THERAPY
• Initial single pill combination therapy with lisinopril-hydrochlorothiazide is preferred. This may be used as initial therapy in all adults.
CKD
• In adults with CKD, regardless of race, consider initial (or add-on) treatment that includes an ACEI or ARB to improve kidney outcomes.
BLACK/AFRICAN AMERICAN
• In Black/African American adults without heart failure or CKD, initial treatment should include a thiazide diuretic or CCB.
CAD, HF, DM
- KP Guideline recommendations for coronary artery disease, heart failure, and DM may inform medication use independent of BP in certain individuals.
THREE MEDICATIONS
- If BP is not controlled within a month of treatment on a thiazide-type diuretic plus ACEI, then add a CCB.
FOUR MEDICATIONS
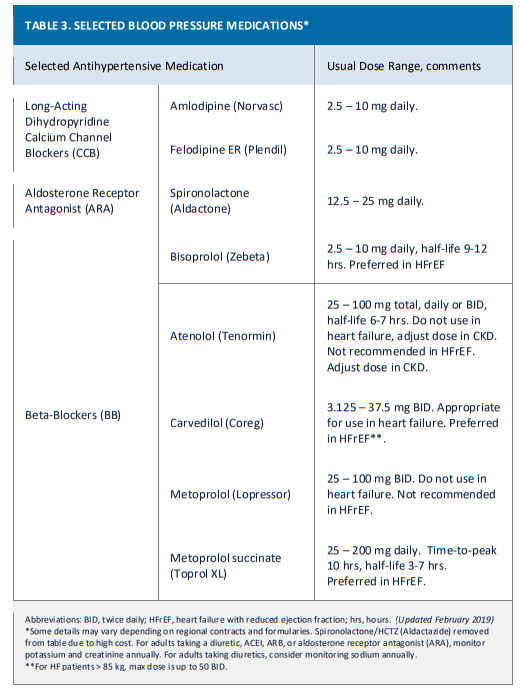
• If BP is not controlled within a month of treatment on a thiazide-type diuretic plus ACEI plus CCB, then add spironolactone (if on thiazide AND eGFR ≥ 60mL/min/1.73 m2 AND potassium < 4.5 mEq/L). If criteria for use of spironolactone are not met, use beta
blocker as fourth agent.WOMEN OF CHILDBEARING POTENTIAL
• Half of all pregnancies are unplanned. Do not prescribe medications contraindicated in pregnancy, such as ACEIs/ARBs, to women of childbearing potential, unless there is a compelling indication. For women of childbearing potential taking medications
contraindicated in pregnancy, such as ACEIs/ARBs:o Discuss potential risks to the fetus if they become pregnant. Discuss practicing contraceptive measures with extremely low failure rates (sterilization, implant, or IUD).
o Advise women using ACEIs/ARBs to stop these medications and advise all women with hypertension to contact their OB/GYN provider immediately if they become pregnant.MONITORING
• In adults with controlled hypertension, monitor BP at least annually.
• Self-monitoring of BP and team-based care can help achieve BP control.
LIFESTYLE, OTHER RISK FACTORS, AND ADHERENCE
LIFESTYLE• In adults with BP ≥ 120/80 mmHg:
o A low sodium, high potassium, heart-healthy diet, such as the DASH (Dietary Approaches to Stop Hypertension) diet is recommended.
o Increased physical activity with a structured exercise program is recommended.
o Weight loss in adults who are overweight or obese is recommended.
o Men and women who currently consume alcohol should be advised to drink no more than 2 and 1 standard drinks* per day, respectively.*In the United States, 1 standard drink contains approximately 14 g of pure alcohol, typically found in 12 oz of regular beer (approximately 5% alcohol), 5 oz of wine (approximately 12% alcohol), and 1.5 oz of distilled spirits (approximately 40% alcohol).
OTHER RISK FACTORS
• To further promote vascular health, follow KP Guidelines to treat cholesterol and diabetes mellitus, recommend aspirin use, and promote tobacco cessation.
ADHERENCE
• Encourage adherence to medications and monitoring. Help overcome barriers.
o Once-daily and combination pills can help minimize pill burden (number of daily pills needed), number of medication copays, and inconvenience.
o Explore and help overcome barriers to medication adherence and monitoring.
Collaborate with patients, families, caregivers, and the care team to problem
solve and implement solutions.
o Address depression and anxiety issues to maximize patient adherence. See KP
National Depression Guideline.
o Educate patients about their goal BP because patients who are knowledgeable
about their goal BP are more likely to achieve it.

ABOUT THIS RESOURCE
This Clinician Guide is based on the 2019 KP National Blood Pressure (BP) Guideline. It was developed to assist primary care physicians and other health care professionals in the outpatient setting with screening and treatment of elevated BP in non-pregnant adults aged ≥ 18 years. The KP National BP Guideline was revised after review of the 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults. It is not intended or designed as a substitute for the reasonable exercise of independent clinical judgment by practitioners.
• Last Review: February 2019
• Next Review: February 2021
\\



