
_____________________________________________________________
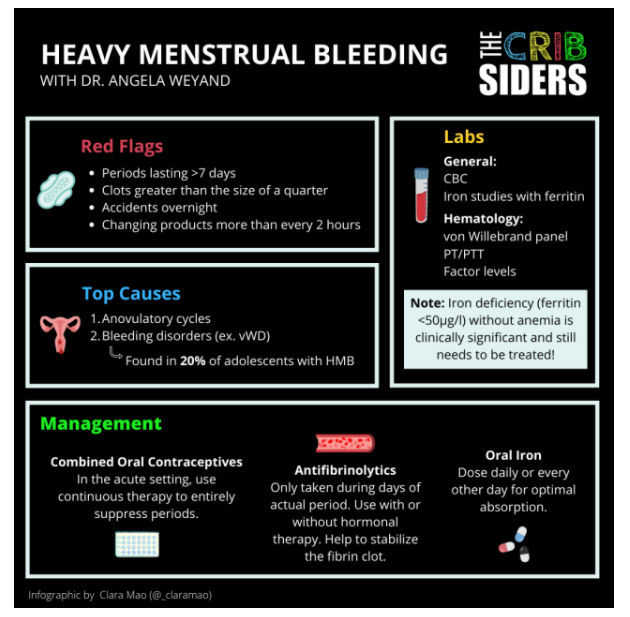
Note to myself: I recommend instead of reviewing the PedsCases resource below, review The Cribsiders‘ [Link is to the episode lis] #40: Period Problems: Heavy Menstrual Bleeding
DECEMBER 8, 2021 By SAM MASUR
Here is the infographic from the above resource:
And although teenage anovulatory dysfunction is seldom due to Polycystic Ovarian Dysfunction, I strongly suggest reviewing The Curbsiders’ #198 PCOS: Polycystic Ovary Syndrome with Katherine Sherif MD.
MARCH 9, 2020 By MOLLY HEUBLEIN
Here are the infographics from the above resource.
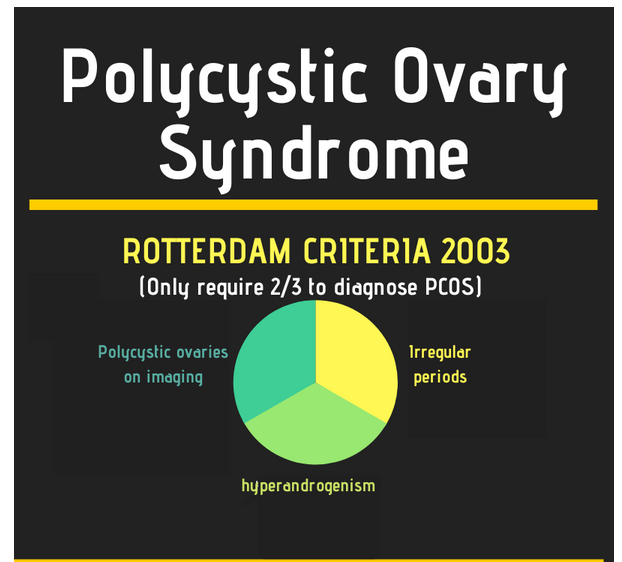
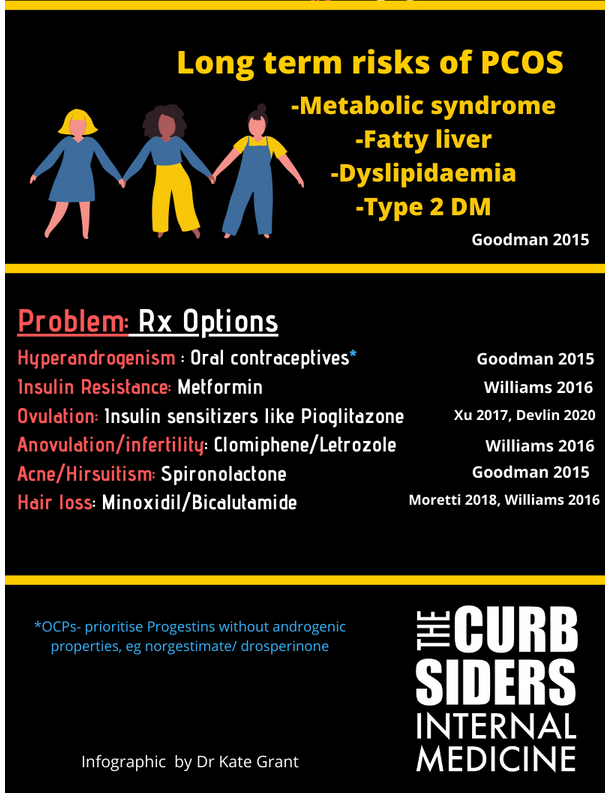
PCOS Infographic pg1 by Kate Grant The Curbsiders #198 PCOS with Katherine Sherif MD
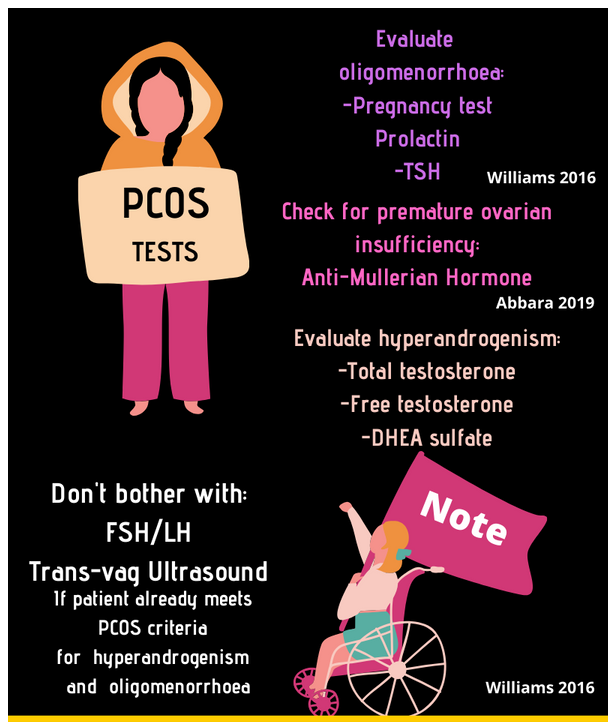
PCOS Infographic pg2 by Kate Grant The Curbsiders #198 PCOS with Katherine Sherif MD
PCOS Pearls
- To diagnose PCOS, patients need any 2 of the following 3: oligomenorrhea, hyperandrogenism, and/or polycystic ovaries seen on imaging
- The underlying cause of PCOS is controversial, but may be related to abnormal hypothalamic-pitutitary-ovarian signaling or primary insulin resistance.
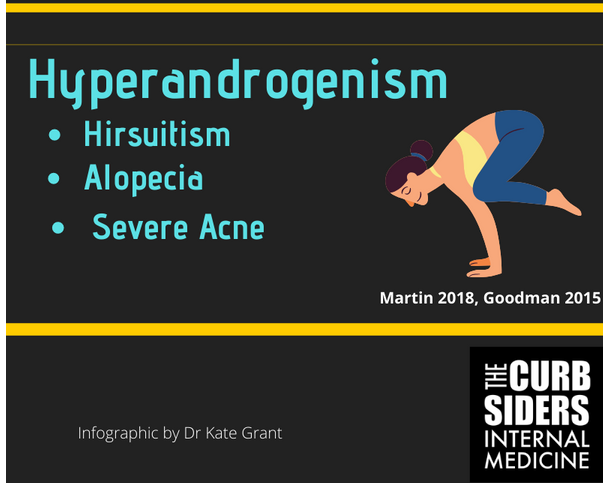
- PCOS can manifest with many dermatologic complaints including hirsutism, alopecia, and acne related to hyperandrogenism and acanthosis nigricans, skin tags, and hidradenitis suppurativa related to insulin resistance
- Treatment for PCOS can include oral contraceptive pills, androgen blockers, and/or insulin sensitizing medications.

______________________________________________________
In this post, I link to and excerpt from PedsCases‘ Abnormal Uterine Bleeding In Adolescents. By Sarah.Moor Jan 10, 2022.
All that follows is from the above resource.
This podcast presents an approach to Abnormal Uterine Bleeding in Adolescents. Listeners will learn about the definition of abnormal uterine bleeding, generate an organized differential diagnosis for abnormal uterine bleeding, and review investigations and management for abnormal uterine bleeding in adolescent patients compared to adult patients. This podcast was developed by Sarah Moor, a third-year medical student at Yale School of Medicine, with Dr. Amanda Kallen, an Assistant Professor of Obstetrics and Gynecology at Yale School of Medicine and member of the Reproductive Scientist Development Program.
Related Content
- Podcast: Adolescent Pregnancy
- Podcast: Sexually Transmitted Infections in Adolescents
- Podcast: Adolescent Medicine
- Podcast: Social History Taking (Part1)
- Podcast: Social History Taking (Part 2)
Differential Diagnosis
When developing our differential, we want to first determine if this is pregnancy or non-pregnancy related bleeding, so it is important to obtain a urine pregnancy test. In our patient, the urine pregnancy test is negative, so this represents non-pregnancy related abnormal uterine bleeding.
For causes of abnormal uterine bleeding we use the acronym PALM-COEIN – polyps, adenomyosis, leiomyoma, malignancy, coagulopathy, ovulatory dysfunction, endometrial,
iatrogenic and not yet classified. In adolescents, structural problems are very rarely the cause of abnormal uterine bleeding, this makes the first half of our acronym PALM, move lower down on our differential.The COEIN part of our acronym then forms the basis for our differential: coagulopathies, such as von Willebrand disease. Ovulatory dysfunction, namely anovulatory cycles, is our O in the acronym and is the most common cause of heavy menstrual bleeding in adolescents as the hypothalamic-pituitary-ovarian axis can still be immature (2). Ovulatory dysfunction is
characterized by irregular, prolonged, and heavy menstrual bleeding. In adolescents, anovulatory dysfunction is physiologic as the HPO axis continues to mature, but later in life it
can be pathologic and is often associated with endocrine abnormalities associated, such as PCOS.*
*The Curbsiders’ #198 PCOS: Polycystic Ovary Syndrome with Katherine Sherif MD.
MARCH 9, 2020 By MOLLY HEUBLEIN
In normal menstruation, the corpus luteum is formed after ovulation and begins releasing progesterone which stabilizes the endometrium. In anovulatory cycles, the corpus luteum is not
formed so there is a decrease in progesterone production which leads to continued endometrial proliferation. However, this endometrial tissue is unstable and tends to shed irregularly. In
addition without progesterone, estrogen is high and unopposed leading to vascular fragility in the endometrium such that a greater volume of blood is lost (4). Endometrial causes, such as
endometrial hyperplasia, are important to keep on the differential, particularly in patients with a personal history of multiple years of untreated anovulatory bleeding and a family history of endometrial, ovarian, breast or colon cancer (5). Iatrogenic in this case is unlikely as the patient is not taking any medications or reporting any previous surgical history. Not otherwise classified keeps us mindful that this acronym is not all-encompassing and to keep our differential open to changes depending on the findings of the workup.The take home points for this discussion are:
1) Abnormal uterine bleeding encompasses bleeding that differs in duration, volume, frequency or regularity from a patient’s baseline. The most common presentation of AUB, particularly in adolescents, is heavy menstrual bleeding.
2) The initial approach to AUB in adolescents is similar to that of adults in that you must determine if this bleeding is occurring in pregnancy or not and whether it is an acute presentation causing hemodynamic instability. However, the approach to gathering this information and to examination in adolescents should be taken more carefully as for adolescents the history and physical exam are particularly sensitive.
3) The underlying etiologies for AUB are described by the mnemonic PALM-COIEN, but structural problems are rare in adolescents so COIEN causes should be prioritized during
the workup for AUB in adolescents.
4) Management of AUB prioritizes treating the underlying cause in addition to the use of hormonal and non-hormonal medical therapies to lower the risk of continued heavy bleeding.



