Google+Links To And Excerpts From The Second E - Ejection From "The "5Es" of emergency physician-performed focused cardiac ultrasound: a protocol for rapid identification of effusion, ejection, equality, exit, and entrance" - Tom Wade MD
Links To And Excerpts From The Second E – Ejection From “The “5Es” of emergency physician-performed focused cardiac ultrasound: a protocol for rapid identification of effusion, ejection, equality, exit, and entrance”
In this post, I link to and excerpt from The Second E-Ejection From The “5Es” of emergency physician-performed focused cardiac ultrasound: a protocol for rapid identification of effusion, ejection, equality, exit, and entrance [PubMed Abstract] [Full-Text HTML] Full-Text PDF]. Acad Emerg Med. 2015 May;22(5):583-93.
All that follows is from the above resource.
Abstract
Emergency physician (EP)-performed focused cardiac ultrasound (EP FOCUS) has been increasingly recognized as a crucial tool to help clinicians diagnose and treat potentially life-threatening conditions. The existing literature demonstrates a variety of EP FOCUS applications and protocols; however, EP FOCUS is not taught, practiced, or interpreted consistently between institutions. Drawing on over 12 years of experience in a large-volume, high-acuity academic emergency department, we have developed a protocol for teaching and performing EP FOCUS known as “The 5Es,” where each E represents a specific assessment for immediately relevant clinical information. These include pericardial effusion, qualitative left ventricular ejection, ventricular equality, exit (aortic root diameter), and entrance (inferior vena cava diameter and respirophasic variation). Each of these assessments has been well described in the emergency medicine literature and is within the scope of EP-performed echocardiography. This approach provides a reliable and easily recalled framework for assessing, teaching, and communicating EP FOCUS findings that are essential in caring for the patient in the emergency setting.
It has been recognized for more than 25 years that emergency physician (EP)-performed focused cardiac ultrasound (EP FOCUS) is an important skill for the care of patients with potentially life-threatening presentations.1, 2 A recent review detailed 16 specific protocols that included cardiac ultrasound (US) as part of the point-of-care US assessment in medical shock.3 The term “focused cardiac ultrasound” has been addressed in some detail (FOCUS,4 FCU,5 and FoCUS6). However, this term is not specialty-specific, may include assessments that are not relevant in the acute/emergency setting, and has not included assessment of the thoracic aortic root (“exit”), which may be particularly applicable to acute and emergent presentations. We have found that the proximal thoracic aorta can be reliably assessed, providing vital information about potential aortic pathology in patients presenting with acute symptoms.7 We thus propose the “5Es” to assess for the presence of a pericardial effusion, left ventricular ejection, ventricular equality, exit (aortic root diameter), and entrance (inferior vena cava [IVC] diameter and respirophasic variation). The 5Es protocol provides an easy-to-teach, evidence-based, and standardized approach to EP FOCUS for the rapid identification and management of time-sensitive pathologic conditions.
Approach to exam
For images in this article, we will use an emergency medicine convention for cardiac imaging with the probe marker oriented to the patient’s right, which keeps the anatomic right on the screen-left, as is the convention for other US imaging.9 This is in contrast with image and probe orientation utilized in traditional cardiology-performed US, but has been recognized as an accepted convention that we find to be conceptually easier, particularly when performing EP FOCUS as part of an integrated examination such as the focused assessment with sonography for trauma (FAST) or the rapid US for shock and hypotension.3, 6
As has been discussed previously in the emergency US literature, EP FOCUS is not intended to replace comprehensive echocardiography (echo) when more thorough cardiology evaluation is indicated. The clinical questions addressed by EP FOCUS tend to be limited and qualitative but it should be understood that EP FOCUS findings may fall on a spectrum that can make binary categorization challenging. The EP is encouraged to use professional judgment for the interpretation and integration of his or her findings into the diagnosis and care of the patient, as well as the need for specialist consultation.
Ejection
The second “E” in our protocol is assessment of LV ejection fraction (LVEF). This E can help differentiate causes of hypotension, chest pain, and dyspnea and may aid in expediting condition-specific therapies.3, 25, 26
There are multiple quantitative modalities for LVEF calculation; however, qualitative estimates of ejection fraction by EP FOCUS correlate well with both quantitative measurements and subjective estimates by cardiologists.25, 27 Qualitative assessment of global ejection is typically categorized as “hyperdynamic” (LVEF > 65%), “normal” (LVEF 50% to 65%), “moderately depressed” (LVEF 30% to 50%), or “severely depressed” (LVEF < 30%).25, 28 Additionally, in cardiac arrest patients, one can recognize “no coordinated myocardial activity” as a likely indicator of futility of further resuscitation.29 Hyperdynamic states are typically associated with decreased afterload, and are most commonly found in patients with sepsis or severe hypovolemia. A severely depressed ejection fraction, particularly when paired with a plethoric IVC (and/or B-lines on thoracic images), indicates systolic heart failure.
Techniques for Assessing Ejection Fraction
For a visual determination of LVEF, the PSLA view is an excellent initial window. The PSLA includes the septum, apex, and posterior LV wall. Additionally, the PSLA view provides good visualization of the anterior leaflet of the mitral valve, allowing for assessment of E-point septal separation (EPSS). Movement of the anterior leaflet of the mitral valve so that it nearly touches the septum in diastole correlates with good LV filling and thus a good ejection fraction.30 EPSS may be assessed by visual estimation or measured quantitatively using B-mode or M-mode to measure the smallest distance from the anterior mitral valve tip to the septal wall during diastole (Figure 3). EPSS measurements greater than 7 mm have been shown to correlate with severely depressed LVEF.31 Rotating from the PSLA to a PSSA view at the level of the papillary muscles shows the entire circumference of the muscular portion of the LV.32 This is an optimal window to observe the concentric squeeze of the LV by estimating the degree of internal chamber collapse in systole versus diastole. This view is also useful to detect focal wall motion abnormalities. In a PSSA view proceeding in a clockwise direction, the septal, anterior, lateral, posterior, and inferior wall segments of the mid-portion of the LV are visible (mnemonic “SALPI”).
The A4C window also provides a good view of the global function of the myocardium, but should include an apical two-chamber view to evaluate all parts of the myocardium. The subxiphoid views may also provide information about global myocardial function, but it may be difficult to see all portions of the LV.
Pearls and Pitfalls of Ejection Fraction
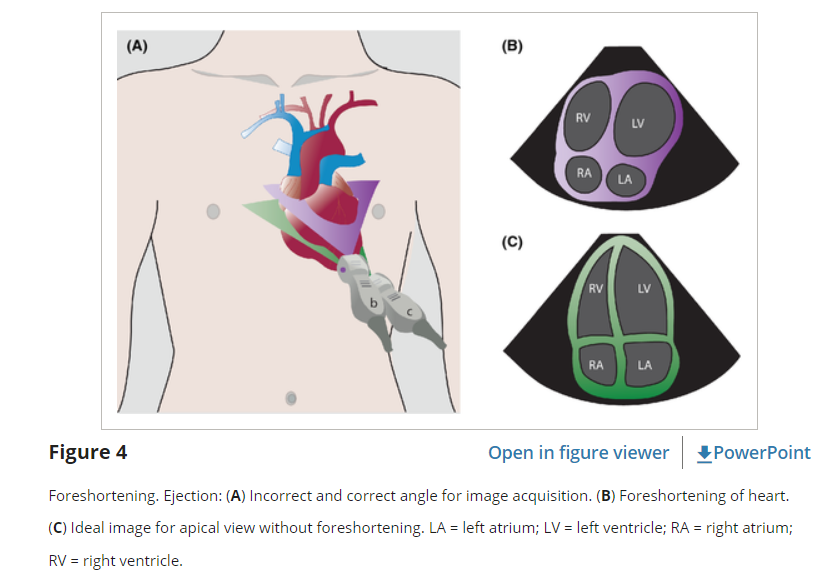
While EPs are very good at distinguishing normal function from severe dysfunction, moderate LV dysfunction can be more difficult to reliably discern.25 It is important to optimize the LV view at the widest diameter of the LV chamber with clearly visible endocardial borders. Being oblique to the LV chamber may underestimate its size and overestimate its emptying (Figure 4). EPSS is a good surrogate measure of ejection fraction, but can be confounded by septal hypertrophy, mitral valve stenosis, or mismeasurements. Two-dimensional images (especially in the A4C view) can be limited by poor lateral resolution and decreased visualization of endocardial borders.31
While the basic EP FOCUS assessment is for estimation of global ejection fraction, focal wall motion abnormalities can affect overall function and represent a pitfall if not appropriately recognized or characterized. Incomplete visualization of all portions of the LV can result in missed focal wall motion abnormalities. When present, these typically indicate myocardial dysfunction or scarring from ischemia, which may be acute or chronic. Myocardial contraction should be observed for several heartbeats, particularly if there are premature ventricular contractions or underlying arrhythmias, such as atrial fibrillation.
Even with a preserved ejection fraction, heart failure still remains a possible cause of dyspnea. Approximately half of all heart failure cases may have some component of impaired relaxation leading to diastolic dysfunction, also known as heart failure with preserved ejection fraction.32