In addition to today’s resource, please review
Today, I review, link to, and excerpt from The Canadian Medical Association Journal‘s “Diagnosis and management of early pregnancy loss”. [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. CMAJ. 2024 Oct 14;196(34):E1162-E1168. doi: 10.1503/cmaj.231489.
All that follows is from the above resource.
- How common is early pregnancy loss?
- What are the risk factors?
- What are the symptoms?
- How is early pregnancy loss diagnosed?
- How is early pregnancy loss managed?
- What is the effect of early pregnancy loss on patients and their families?
- Conclusion
- Footnotes
- References
- Associated Data
KEY POINTS
- Early pregnancy loss, also known as miscarriage, is common, distressing, and frequently poorly managed in Canada.
- Diagnosis of early pregnancy loss requires determination of serum β-human chorionic gonadotropin (β-hCG) levels and pelvic ultrasonography, preferably transvaginal, to investigate pregnancy viability and distinguish early pregnancy loss from an ectopic pregnancy. [Emphasis added]
- Treatment options include expectant, medical, and surgical management.
- Early pregnancy loss can have devastating psychological effects, which may be mitigated by empathetic communication and supportive follow-up.
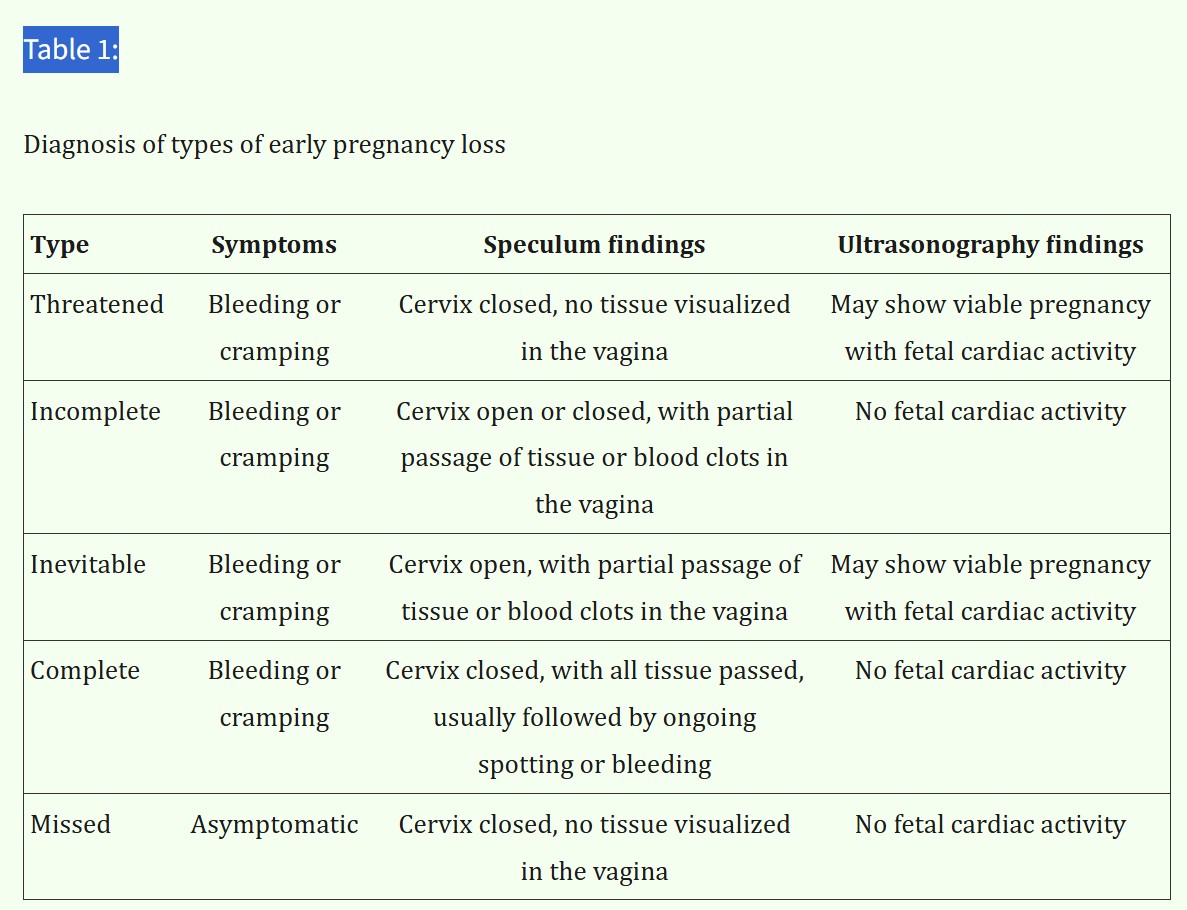
Early pregnancy loss is common and often devastating. Adverse medical and psychological complications may be avoided with the provision of informed, compassionate care. Also known as miscarriage, early pregnancy loss is defined as an empty gestational sac or a gestational sac with embryo without fetal cardiac activity before 13 weeks’ gestation.1 Early pregnancy loss can be further divided into incomplete, complete, and missed, which can be diagnosed based on findings from physical examination and pelvic ultrasonography (Table 1). If the location of the pregnancy is not confirmed, an ectopic pregnancy must be ruled out. [Emphasis added]
We summarize the best available evidence on the prevalence, risk factors, presentation, diagnosis, compassionate management, and follow-up of early pregnancy loss (Box 1).
How common is early pregnancy loss?
The incidence of early pregnancy loss differs globally, in part because of varying definitions. Prospective data from Europe and North America suggest early pregnancy loss affects 15%–20% of all clinically recognized pregnancies.2 The reported incidence was even higher (31%) when pregnant people were followed with serial testing of serum β-human chorionic gonadotropin (β-hCG) in early pregnancy.3 Many pregnancies are lost before the patient recognizes they are pregnant, and signs of early pregnancy loss may be mistaken for late or heavy menses.3 In Canada, 2 population-based retrospective cohort studies have informed incidence estimates, with early pregnancy loss in 8.1% and 10.1%–12.5% of recognized pregnancies in Ontario and Manitoba, respectively.4,5 Interprovincial differences make it challenging to determine the actual incidence of early pregnancy loss in Canada or to compare it with that of other countries.
What are the risk factors?
Around half of all early pregnancy losses are a result of chromosomal abnormalities in the developing embryo, such as aneuploidy.6 Maternal age older than 35 years significantly increases the risk of early pregnancy loss; among people aged 45 years or older, this risk is nearly 65%.2,7 Other risk factors include a history of early pregnancy loss, infection with pathogens such as Chlamydia trachomatis, older paternal age, extremes in body mass index, smoking, alcohol consumption, physical trauma, psychological stress, exposure to air pollution, and pesticide exposure.2,8–10 An association between early pregnancy loss and being Black has also been reported and is thought to be related to biological (e.g., a greater prevalence of anemia, diabetes, dyslipidemia), genetic (i.e., in genes related to immunological and inflammatory pathways), and socioeconomic factors.11–14
What are the symptoms?
Common symptoms of early pregnancy loss include bleeding, cramping, abdominal or pelvic pain, passage of tissue, or a combination of these. Symptoms of ectopic pregnancy, which should be ruled out, include worsening abdominal pain, dizziness, bleeding, or shoulder-tip pain.15 Septic miscarriage should be suspected in the presence of fever, elevated leukocyte count, pelvic pain, uterine tenderness, or purulent discharge. Patients may also be asymptomatic with a missed early pregnancy loss.
Cramping or pain during pregnancy is common. Nearly 85% of pregnant patients have abdominal pain during the first 7 weeks of pregnancy.15 Vaginal bleeding occurs during the first trimester in 25% of all pregnant patients with normal pregnancy outcomes.16 Studies have shown that the risk of early pregnancy loss is 5 times greater among patients who have both bleeding and cramping (hazard ratio 5.03, 95% confidence interval [CI] 2.07–12.20), compared with those who have cramping only.15
How is early pregnancy loss diagnosed?
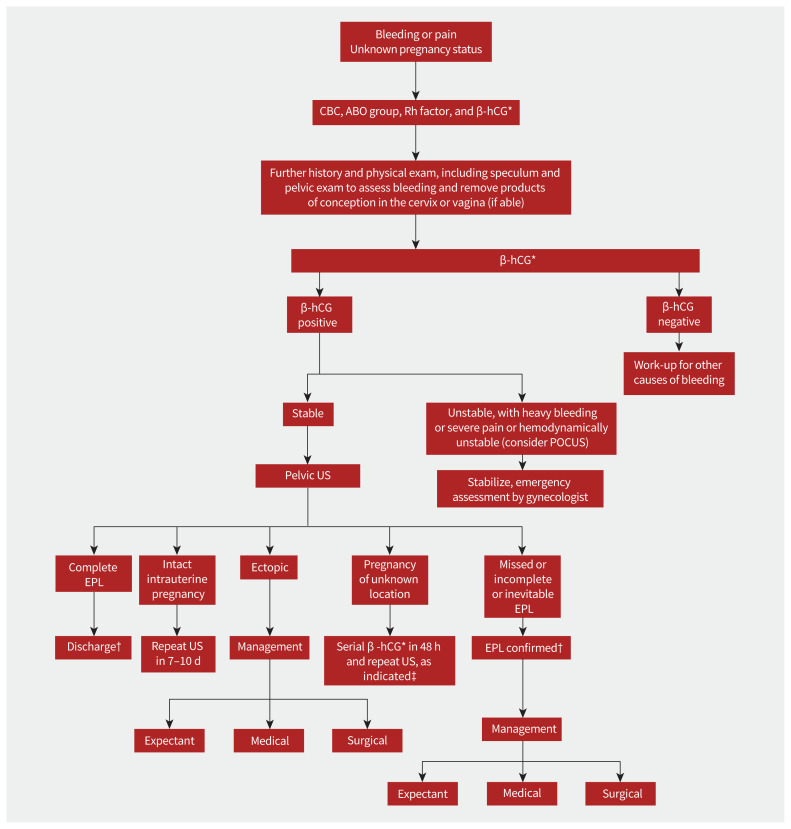
The steps for distinguishing early pregnancy bleeding, or pain related to early pregnancy loss, from other causes are shown in Figure 1. All patients require a detailed history, and a physical exam should be conducted to remove any cervical or vaginal clots to reduce bleeding and help visualize the cervix. Initial investigations include a complete blood count and determination of blood group, Rh factor, and β-hCG levels. Serum β-hCG levels confirm pregnancy, and a baseline level can be established to compare with previous and subsequent values. If a patient is hemodynamically unstable, they should be resuscitated and urgently referred to the gynecology team.1 Once the patient is stable, ultrasonography should be performed, preferably transvaginally.
Diagnosis of early pregnancy loss. *Quantitative β-human chorionic gonadotropin (β-hCG) is preferred if available, but qualitative or urine β-hCG can be used if a quantitative measure is unavailable. †Patient should be offered patient-centred compassionate treatment and resources in the community. ‡The ratio of repeat β-hCG to initial β-hCG can stratify risk of ectopic pregnancy and will determine the need and timing of serial ultrasonography. See Related Content tab for accessible version. Note: CBC = complete blood count, EPL = early pregnancy loss, POCUS = point-of-care ultrasonography, US = ultrasonography.
Around 10% of people with symptoms consistent with early pregnancy loss in their first trimester will have elevated serum β-hCG without an identified location of the pregnancy by initial ultrasonography, known as a pregnancy of unknown location.17 This may represent an intrauterine pregnancy (viable or nonviable), a resolving pregnancy of unknown location (where the location is never identified), or a persisting pregnancy of unknown location, which must be followed until an ectopic pregnancy can be ruled out. The incidence of pregnancy of unknown location is around 15% among pregnant people undergoing routine transvaginal ultrasonography early in the first trimester.17 Patients with pregnancy of unknown location and symptoms of early pregnancy loss have an 8%–14% risk of ectopic pregnancy, and empirical medical or surgical intervention is inappropriate without further investigation.18
For hemodynamically stable patients, a repeat serum β-hCG should be obtained at 48 hours. The ratio of repeat β-hCG to initial β-hCG can stratify risk of ectopic pregnancy.17 A ratio greater than 1.63 suggests an intrauterine pregnancy, and the patient should have repeat transvaginal ultrasonography 1 week later. A ratio below 0.5 indicates a failing pregnancy that will resolve naturally, without need for repeat ultrasonography. Ratios between 0.5 and 1.63 suggest ectopic pregnancy and require close follow-up with repeat ultrasonography and β-hCG in 48 hours; a gynecologist should be consulted.17 Other risk stratification tools, such as the M6 Regression Model, are beneficial but are not yet widely used in Canada.18 Expectant management of pregnancy of unknown location is generally safe when risk of ectopic pregnancy is low, but close follow-up with a health care provider is critical until the β-hCG level becomes undetectable.