Please see also 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines [PubMed Abstract]. Circulation. 2022 Jan 18;145(3):e4-e17.
In this post, I link to and excerpt from 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. J Am Coll Cardiol. 2022 Jan 18;79(2):e21-e129.
All that follows is from the above resource.
Abstract
Aim
The guideline for coronary artery revascularization replaces the 2011 coronary artery bypass graft surgery and the 2011 and 2015 percutaneous coronary intervention guidelines, providing a patient-centric approach to guide clinicians in the treatment of patients with significant coronary artery disease undergoing coronary revascularization as well as the supporting documentation to encourage their use.
Structure
Coronary artery disease remains a leading cause of morbidity and mortality globally. Coronary revascularization is an important therapeutic option when managing patients with coronary artery disease. The 2021 coronary artery revascularization guideline provides recommendations based on contemporary evidence for the treatment of these patients. The recommendations present an evidence-based approach to managing patients with coronary artery disease who are being considered for coronary revascularization, with the intent to improve quality of care and align with patients’ interests.
Top 10 Take-Home Messages
- 1.
Treatment decisions regarding coronary revascularization in patients with coronary artery disease should be based on clinical indications, regardless of sex, race, or ethnicity, because there is no evidence that some patients benefit less than others, and efforts to reduce disparities of care are warranted.
- 2.
In patients being considered for coronary revascularization for whom the optimal treatment strategy is unclear, a multidisciplinary Heart Team approach is recommended. Treatment decisions should be patient centered, incorporate patient preferences and goals, and include shared decision-making.
- 3.
For patients with significant left main disease, surgical revascularization is indicated to improve survival relative to that likely to be achieved with medical therapy. Percutaneous revascularization is a reasonable option to improve survival, compared with medical therapy, in selected patients with low to medium anatomic complexity of coronary artery disease and left main disease that is equally suitable for surgical or percutaneous revascularization.
- 4.
Updated evidence from contemporary trials supplement older evidence with regard to mortality benefit of revascularization in patients with stable ischemic heart disease, normal left ventricular ejection fraction, and triple-vessel coronary artery disease. Surgical revascularization may be reasonable to improve survival. A survival benefit with percutaneous revascularization is uncertain. Revascularization decisions are based on consideration of disease complexity, technical feasibility of treatment, and a Heart Team discussion.
- 5.
The use of a radial artery as a surgical revascularization conduit is preferred versus the use of a saphenous vein conduit to bypass the second most important target vessel with significant stenosis after the left anterior descending coronary artery. Benefits include superior patency, reduced adverse cardiac events, and improved survival.
- 6.
Radial artery access is recommended in patients undergoing percutaneous intervention who have acute coronary syndrome or stable ischemic heart disease, to reduce bleeding and vascular complications compared with a femoral approach. Patients with acute coronary syndrome also benefit from a reduction in mortality rate with this approach.
- 7.
A short duration of dual antiplatelet therapy after percutaneous revascularization in patients with stable ischemic heart disease is reasonable to reduce the risk of bleeding events. After consideration of recurrent ischemia and bleeding risks, select patients may safely transition to P2Y12 inhibitor monotherapy and stop aspirin after 1 to 3 months of dual antiplatelet therapy.
- 8.
Staged percutaneous intervention (while in hospital or after discharge) of a significantly stenosed nonculprit artery in patients presenting with an ST-segment–elevation myocardial infarction is recommended in select patients to improve outcomes. Percutaneous intervention of the nonculprit artery at the time of primary percutaneous coronary intervention is less clear and may be considered in stable patients with uncomplicated revascularization of the culprit artery, low-complexity nonculprit artery disease, and normal renal function. In contrast, percutaneous intervention of the non-culprit artery can be harmful in patients in cardiogenic shock.
- 9.
Revascularization decisions in patients with diabetes and multivessel coronary artery disease are optimized by the use of a Heart Team approach. Patients with diabetes who have triple-vessel disease should undergo surgical revascularization; percutaneous coronary intervention may be considered if they are poor candidates for surgery.
- 10.
Treatment decisions for patients undergoing surgical revascularization of coronary artery disease should include the calculation of a patient’s surgical risk with the Society of Thoracic Surgeons score. The usefulness of the SYNTAX score calculation in treatment decisions is less clear because of the interobserver variability in its calculation and its absence of clinical variables.
1.4. Scope of the Guideline
The scope of the “2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization” is to provide an update to and to consolidate the 2011 coronary artery bypass graft (CABG) surgery (1) and the 2011 and 2015 percutaneous coronary intervention (PCI) guidelines (2,3), with the added consideration of using a patient-centric disease approach. The applicable sections on revascularization from the 2012 stable ischemic heart disease (SIHD) guideline (4), as well as the 2013 ST-segment–elevation myocardial infarction (STEMI) (5) and 2014 non–ST-segment–elevation myocardial infarction (NSTEMI) guidelines (6), will also be updated. This present guideline will affect the following documents:
- 1.
Replace/retire the 2011 PCI guideline (2).
- 2.
Replace/retire the 2011 CABG guideline (1).
- 3.
Replace/retire the 2015 update in PCI in STEMI guideline (3).
- 4.
Replace/retire the 2013 STEMI guideline, Sections 4.1, 4.2, 4.3, 4.4, 5.3 (deals with transfer after lytic with intent to do PCI), 6.2, 6.4, 7.1, and 7.2 (5).
- 5.
Replace/retire 2014 non–ST-segment–elevation acute coronary syndrome (NSTE-ACS) guideline, Sections 4.4.4, 5.1.1, 5.1.2.1, 5.1.2.2, 5.1.2.3, and 5.2 (6).
- 6.
The intended primary target audience consists of cardiovascular clinicians who are involved in the care of patients for whom revascularization is considered or indicated. Coronary artery disease (CAD) is to be approached with the most current treatment options and treated as a “condition.” Recommendations are stated in reference to the patients and their condition. The focus is to provide the most up-to-date evidence to inform the clinician during shared decision-making with the patient. Although the document is not intended to be a procedural-based manual of recommendations that outlines the best practice for coronary revascularization, there are certain techniques that surgeons or interventional cardiologists might use that are associated with improved clinical outcomes.
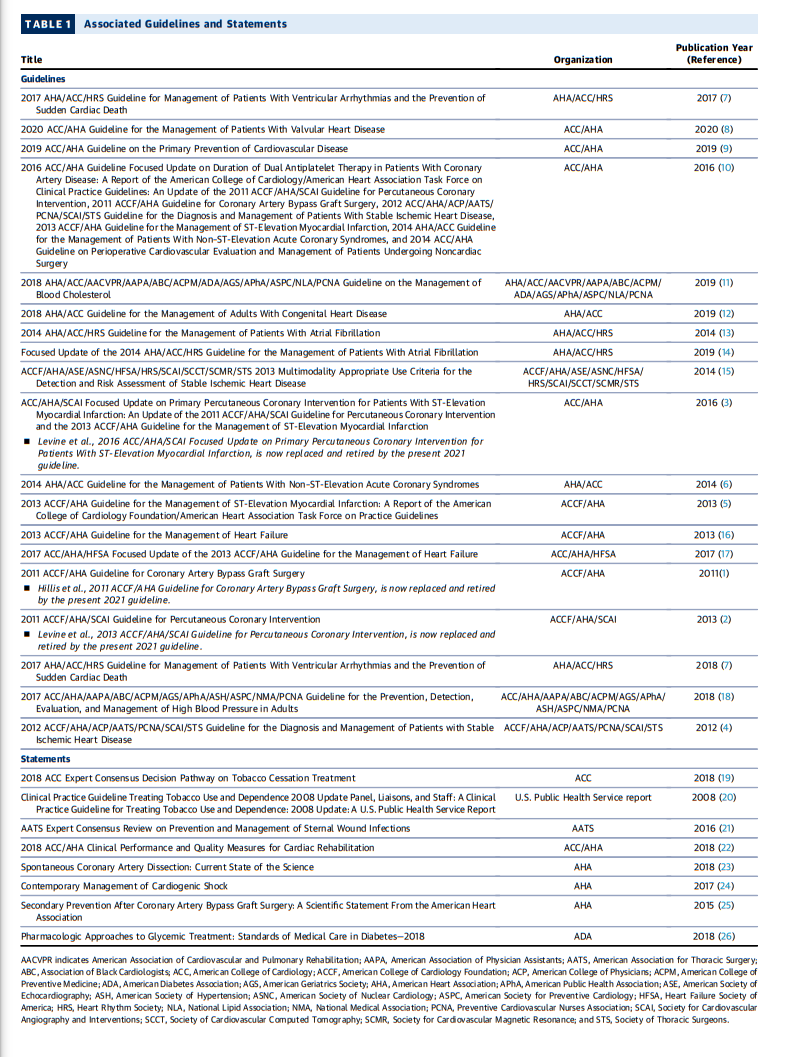
In developing the 2021 coronary artery revascularization guideline, the writing committee reviewed previously published guidelines and related statements. Table 1 contains a list of these publications and statements deemed pertinent to this writing effort and is intended for use as a resource, thus obviating the need to repeat existing guideline recommendations.
Start here.