
In this post I link to and excerpt from FOAMcast’s May 16, 2018 Pulmonary Embolism Risk Stratification and ACEP Clinical Policy. Here is the link to the podcast and here is the link to the show notes.
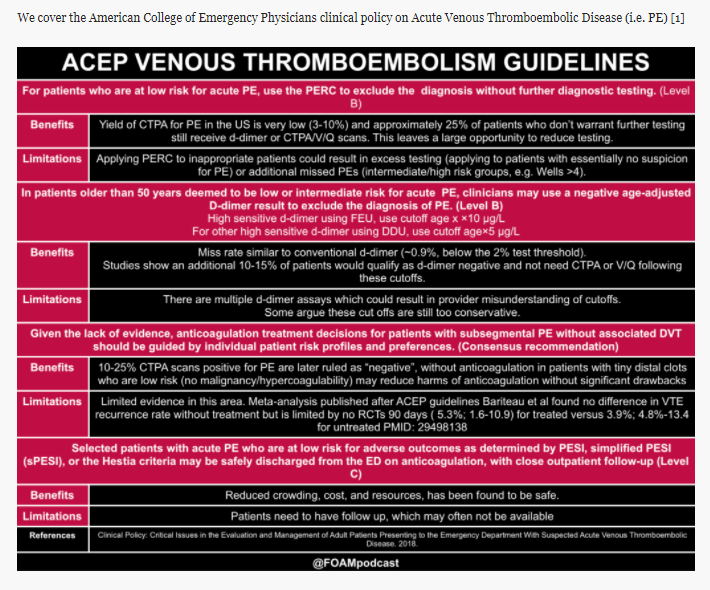
Here are links to American College of Emergency Physicians clinical policy on Acute Venous Thromboembolic Disease [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Ann Emerg Med. 2018 May;71(5):e59-e109..
Here are excerpts from the FOAMcast show notes [As always I place these here as doing so helps me reinforce my learning].
Risk Stratification in Pulmonary Embolism
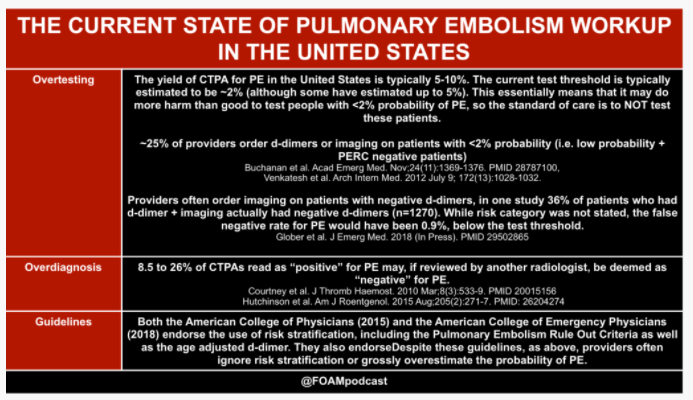
In the United States, the workup rate for PE is astonishingly high, with 1-2% of all ED patients receiving a CTPA for PE and a low yield (~5-10% of CTPAs are positive for PE). Thus, major medical societies such as ACEP and the American College of Physicians recommend the use of risk stratification tools [1,2]. For some reason, approximately 25% of patients who are low risk AND PERC negative still receive d-dimer or imaging for PE, despite the risk of PE being exceptionally low. To be clear, use of clinical decision tools are not mandatory and do not necessarily perform better than clinical gestalt [9]. These tools may serve as a “reality check” for some, reminding them that patients may be at lower risk of PE than they think.

text

Text
Podcast: Play in new window | Download



