
The following are excerpts from resource (1):
1 Characterization of Coronary Spasm in Ischemic Heart Disease
(1) Characterization of Coronary Spasm in Terms of
the Etiology of AnginaIn coronary spasm, sudden excessive coronary vasoconstriction
produces a transient reduction of blood flow, resulting
in myocardial ischemia (supply ischemia/primary angina).
Although coronary spasm occurs mainly in large coronary
arteries running on the surface of the heart, it is also known to
occur in the coronary microvasculature of the myocardium.
Coronary spasm is not always preceded by elevations of blood
pressure and heart rate, which increase myocardial oxygen
consumption. In this regard, coronary spasm is a pathological
condition that is clearly distinguishable from demand
ischemia/secondary angina represented by effort angina.
Coronary spasm develops in sclerotic lesions of varying
severity. Even when no stenotic lesions are visible on coronary
angiography, intravascular ultrasound (IVUS) reveals
clear arteriosclerotic lesions in locations consistent with
regions of coronary spasm.5 Reduction of blood flow due to
coronary spasm activates platelets and the coagulation
system,6 causing vascular smooth muscle cell proliferation.7
It has in fact been revealed by evaluation using quantitative
coronary angiography that the locations of coronary spasm
induced in provocation tests were particularly susceptible to
progression of arteriosclerosis.8,9(2) Characterization of Coronary Spasm in Acute
Coronary SyndromeIt was reported as early as the 1970s that coronary spasm can
trigger not only angina but also myocardial infarction. There
have been patients with acute myocardial infarction in whom
emergent coronary angiography revealed extremely mild
organic stenosis, as well as patients with complete coronary
occlusion which exhibited recanalization after administration
of nitrates alone. Recently, unstable angina, acute
myocardial infarction, and sudden ischemic cardiac death
have been referred to collectively as acute coronary
syndrome. This is because these diseases share the pathological
finding of rapid progression of coronary lesions, ie,
disruption of coronary atheroma (plaque) and the resulting
thrombus formation.10 Coronary plaques are observed in the
form of local thickening of the intima, and are structurally
characterized by the accumulation of foamy macrophages
forming a lipid core covered by a fibrous cap of connective
tissue and smooth muscle cells. It has been hypothesized
that if a tear occurs in this cap, the highly thrombogenic
plaque content becomes exposed to the blood flow and
rapidly forms thrombi that obstruct the vascular lumen.
Plaques more likely to be ruptured are termed vulnerable
plaques; they are often characterized by high lipid content
and a thinned fibrous cap, and tend to be large.
It has been suggested that coronary spasm is a cause of
rupture of vulnerable plaques. Investigations of coronary
lesions in autopsies have demonstrated that spasm causes
endothelial cell derangement and fibrous cap rupture, resulting
in the protrusion of the plaque content exposed to the
vascular lumen, where thrombi are produced.11 In addition,
coronary spasm is accompanied by hypercoagulation,12
decreased fibrinolytic activity,13 and activation of platelets
and adhesion molecules,14 resulting in a thrombophilic state
in acute coronary syndrome. Although plaque stabilization
(prevention of rupture) and antithrombotic therapy are
important in the prevention and treatment of acute coronary
syndrome, prevention of coronary spasm is also important,
particularly in Japanese, in whom the prevalence of coronary
spasm is higher than in western countries.2 Diagnostic Criteria
At present, vasospastic angina is diagnosed in Japan using
criteria independently adopted by individual institutions. In
this background, the present guidelines are established to
unify the diagnostic criteria with reference to previous
reports and other findings. Yasue et al. state that vasospastic
angina can be diagnosed even without performing coronary
angiography, provided that anginal attacks disappear quickly
upon administration of nitroglycerin, and that any one of the
five conditions shown below is met:(1) attacks appear at rest, particularly between night and early morning;
(2)marked diurnal variation is observed in exercise tolerance (in particular, reduction of exercise capacity in the early morning);
(3) attacks are accompanied by ST elevation on
the ECG;(4) attacks are induced by hyperventilation (hyperpnea);
(5) attacks are suppressed by calcium channel blockers but not by β-blockers.15 In the present guidelines, reference
items based on that opinion are included in the
diagnostic criteria established for three grades: “Definite,”
“Suspected,” or “Unlikely”. The diagnostic criteria for vasospastic angina are provided below. A diagnostic flow chart is shown in Figure 1.
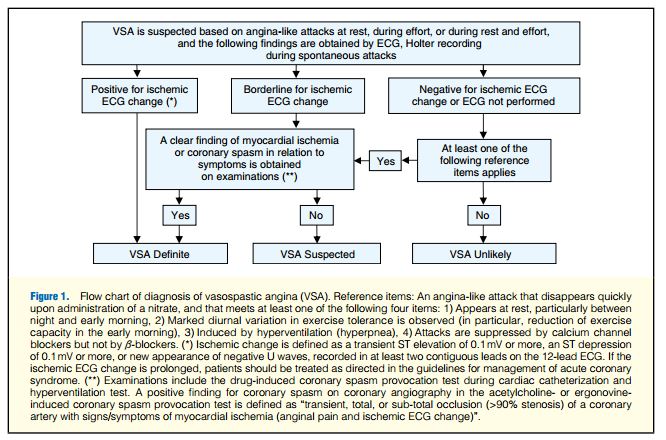
Diagnostic Criteria for “Definite/Suspected” Vasospastic Angina
If any one of the following conditions and one of the following
requirements are met, Definite/Suspected vasospastic
angina is considered present. If none of them is met, the
condition is judged Unlikely to be vasospastic angina.
Clinically, both Definite and Suspected vasospastic angina
are diagnosed as vasospastic angina.
Conditions (any one of the three below)1. Spontaneous attacks
2. Positive non-drug-induced coronary spasm provocation
test (eg, hyperventilation test and exercise test)
3. Positive drug-induced coronary spasm provocation test
(eg, acetylcholine provocation test and ergonovine provocation test)Requirements
A. “Definite vasospastic angina”
The patient is considered to have Definite vasospastic
angina when ischemic change is clearly observed on the
ECG during attacks (*); when the ECG findings are
borderline but a clear finding of myocardial ischemia or
coronary spasm is obtained in examinations (**) and he/
she has a history and symptoms during attacks that are consistent with vasospastic angina; or when, if there is no
ECG change during attacks or if ECG examination has
not been performed, at least one of the following reference
items is met, and examinations (**) reveal a clear
finding of myocardial ischemia or coronary spasm.
B. “Suspected vasospastic angina”
The patient is considered to have Suspected vasospastic
angina when the ischemic change on ECG during attacks
is in the borderline, and no clear finding of myocardial
ischemia or coronary spasm is obtained in any examination
(**); or when, if there is no change on the ECG during
attacks or ECG examination has not been performed, one
or more of the following reference items apply, and a clear
finding of myocardial ischemia or coronary spasm cannot
be demonstrated on any examination (**).
(*) Ischemic change is defined as a transient ST elevation
of 0.1mV or more, an ST depression of 0.1mV or more,
or new appearance of negative U waves, recorded in at
least two contiguous leads on the 12-lead ECG. If the
ischemic ECG change is prolonged, patients should be
treated as directed in the guidelines for management of
acute coronary syndrome.
(**) Examinations include the drug-induced coronary
spasm provocation test during cardiac catheterization and
hyperventilation test. A positive finding for coronary
spasm on coronary angiography in the acetylcholine- or
ergonovine-induced coronary spasm provocation test is
defined as “transient, total, or sub-total occlusion (>90%
stenosis) of a coronary artery with signs/symptoms of
myocardial ischemia (anginal pain and ischemic ECG
change).”16–19Reference Items
An angina-like attack that disappears quickly upon administration of a nitrate, and that meets at least one of the following four items:
1) Appears at rest, particularly between night and early
morning.
2) Marked diurnal variation in exercise tolerance is observed
(in particular, reduction of exercise capacity in the early
morning).
3) Induced by hyperventilation (hyperpnea).
4) Attacks are suppressed by calcium channel blockers but
not by β-blockers.
Etiology and epidemiology are discussed in reference (1) on p 1748 + 1749. These factors include smoking, drinking, lipid abnormalities, stress (abnormal autonomic nervous system function), and genetic factors.
Pathophysiology is discussed in reference (1) on p 1749 + 1750.
(1) Subjective Symptoms (1) Characterized by vague pain that cannot be indicated by
a single finger, with a sensation of compression, a pressing
sensation, and a sensation of tightness in the precordium,
especially in the center of the substernal region.
Occasionally, symptoms develop in the upper abdomen.
(2) Appears at rest, with pain persisting for several to about
15 minutes. The pain often radiates to the neck, jaws,
left shoulder, and elsewhere, occasionally accompanied
by symptoms such as numbness and weakness of the left
shoulder and upper arm.
(3) Anginal attacks due to coronary spasm often persist
longer than effort anginal attacks due to organic stenotic
lesions, and are sometimes accompanied by cold sweats
and disturbance of consciousness including syncope.
(4) Can be induced by hyperpnea and drinking of alcohol.
(5) Fast-acting nitrates are remarkably effective against
attacks of coronary spasm.
(6) Calcium channel blockers suppress attacks of coronary
spasm.
(7) Attacks are often accompanied by arrhythmias; if they
are complicated by complete atrioventricular block,
ventricular tachycardia, or ventricular fibrillation, disturbance of consciousness or syncope is observed.
(8) Attacks of coronary spasm typically occur at rest
between night and early morning. They are usually not
induced by daytime exercise. Diurnal variation with a
peak between night and early morning is observed; 67%
of attacks are asymptomatic episodes of myocardial
ischemia without subjective symptoms (Figure 4).69
Usually, attacks of vasospastic angina can be induced by
even slight effort in the early morning, but are not
induced by even strenuous effort in the afternoon or later
in the day. Hence, diurnal variation is also observed in
exercise tolerance in patients with vasospastic angina.
(9) Attacks of coronary spasm may occur frequently, ie,
several times every day, or may not occur for several
months to several years.
(2) Physical Findings
In auscultation during attacks, gallop rhythms and systolic
murmurs are sometimes heard. These are caused by
decreased wall motion, mitral regurgitation, and other
changes resulting from ischemia. If symptoms disappear
upon administration of a fast-acting nitrate or similar agent,
these findings may also disappear. Hypotension may occur
during attacks. In addition, since the arrhythmias developing
in association with attacks include complete atrioventricular
block, ventricular tachycardia, and ventricular fibrillation,
they must be monitored for carefully.
For methods of evaluation see pp 751 – 1754 of reference (1).
Resources:
(1) Guidelines for Diagnosis and Treatment of Patients With Vasospastic Angina (Coronary Spastic Angina) (JCS 2008)– Digest Version –. [PubMed Citation] [Full Text PDF]. Circ J. 2010 Aug;74(8):1745-62.
(2) Vasospastic Angina. European Society of Cardiology, E-Journal of Cardiology Practice, Volume 2, No9 11 Nov 2003.
(3) Prognostic Stratification of Patients With Vasospastic Angina: A Comprehensive Clinical Risk Score Developed by the Japanese Coronary Spasm Association. [PubMed Abstract] [Full Text HTML] [Download Full Text PDF]. J Am Coll Cardiol. 2013 Sep 24;62(13):1144-53.



