In this post, I link to and excerpt from Version 3 of the Alzheimer Disease Centers’ Neuropsychological Test Battery in the Uniform Data Set (UDS) [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Alzheimer Dis Assoc Disord. 2018 Jan-Mar;32(1):10-17. doi: 10.1097/WAD.0000000000000223.
All that follows is from the above resource.
Abstract
Introduction:
The neuropsychological battery of the Uniform Data Set (UDSNB) was implemented in 2005 by the National Institute on Aging (NIA) Alzheimer Disease Centers program to measure cognitive performance in dementia and mild cognitive impairment due to Alzheimer Disease. This paper describes a revision, the UDSNB 3.0.
Methods:
The Neuropsychology Work Group of the NIA Clinical Task Force recommended revisions through a process of due diligence to address shortcomings of the original battery. The UDSNB 3.0 covers episodic memory, processing speed, executive function, language, and constructional ability. Data from 3602 cognitively normal participants in the National Alzheimer Coordinating Center database were analyzed.
Results:
Descriptive statistics are presented. Multivariable linear regression analyses demonstrated score differences by age, sex, and education and were also used to create a normative calculator available online.
Discussion:
The UDSNB 3.0 neuropsychological battery provides a valuable non proprietary resource for conducting research on cognitive aging and dementia.
Key Words: dementia, neuropsychological test, cognition, UDS
Selection of Tests for the UDS Neuropsychological Battery 3.0
The Work Group recommended replacing the MMSE with the MoCA,16,17 Logical Memory18 immediate and delayed with the Craft Story 21 immediate and delayed recall19; digit span forward and backward with the number span forward and backward test; and the Boston naming test (BNT) with the multilingual naming test (MINT).20 Each decision was based on the rationale outlined below.
General Cognitive Measure
The MoCA16,17 was selected to replace the MMSE as a measure of overall cognitive impairment. Factors influencing this decision included the fact that the MOCA is more difficult than the MMSE as demonstrated in studies showing lower MoCA than MMSE scores in the same samples21 and, hence, more likely to detect subtle cognitive deficits. Furthermore, floor and ceiling effects are less common with the MoCA, which also allows for a broader range of scores in MCI samples than does the MMSE.22 Therefore, the MoCA is more appropriate than the MMSE for detecting early cognitive decline. The MoCA has been validated in white23 and African American24 groups. A disadvantage of the MoCA is that it can yield lower scores in diverse healthy population-based samples.25 However, an abbreviated version reportedly demonstrated predictive ability with respect to diagnosis of MCI in a low-education, illiterate sample.26 In another study, MoCA was more sensitive to MCI and discriminated MCI from other samples better than the MMSE.27,28 MoCA scores have also been shown to correlate with the Activities of Daily Living Questionnaire29 a measure of functional integrity in dementia.30 The MoCA has the further advantage of yielding not only a total score (overall measure) but also index scores based on individual items tapping domains of attention, retentive memory, orientation, language, and executive function.31
The MoCA requires about 10 minutes to administer and yields a total score of 30 and the above-mentioned domain index scores. The index scores (not included in the present report) offer the potential to identify early dementia profiles of clinical dementia subtypes such as behavioral variant frontotemporal dementia and primary progressive aphasia. The memory index score has been shown to be especially predictive of decline from amnestic MCI to AD dementia.31 The paper-and-pencil version of the MoCA has been translated into multiple languages and dialects within languages32 and is freely available (www.mocatest.org/). The NACC was given permission to use it for 25 years without royalties or restrictions on sharing the test with collaborators.
Development of Domain-specific Neuropsychological Tests
Episodic Memory Tests
Memory loss is the hallmark symptom of the most common clinical dementia syndrome associated with AD.33 Early studies of AD dementia emphasized the importance of measures of episodic memory, such as word list learning and story recall, in the evaluation for dementia. The group had decided on a story memory test, as most ADCs were already using Logical Memory, immediate, and delayed recall conditions.
Craft and colleagues had designed multiple forms of a story recall test similar to Logical Memory in a study of the impact of insulin on cognition in mild AD dementia.19,34 The complete set of 22 stories had previously been tested for equivalence in a diverse sample of college age adults who were administered all of the stories in counter balanced order in the laboratory of Andrew Saykin (personal oral communication) and provided to the Work Group for consideration. Additional data on alternate sets of stories were included in published studies of patients undergoing systemic chemotherapy for treatment of breast cancer as well as individuals with traumatic brain injury and healthy controls.35–38 In a pilot study to determine the equivalence of 22 stories in middle-aged and older adults the Work Group determined that 3 stories offered the greatest relationship to Logical Memory and to one another. These 3 were reviewed by the work group and 1 was chosen for its content relevance to a diverse population, “Craft Story 21.”
Scoring of Logical Memory allows several acceptable responses for each item recalled. Following the protocol from Craft et al,34 items were scored in a similar manner to Logical Memory (paraphrase score) but another score was also calculated (verbatim score), allocating a point for each item recalled exactly as delivered in the story. The verbatim score (not included in the present report) was intended to serve as potentially more sensitive than the paraphrase score in detecting very early memory decline.
Finally, we introduced a novel measure of nonverbal memory, a function not previously included in the UDSNB 2.0. Following the copy of the Benson complex39 figure (see the Visuospatial Test section) delayed figure reproduction was tested.
Language Tests
The 32-item MINT20,40 was selected to replace the short BNT. The MINT was originally developed to test naming in 4 languages, English, Spanish, Hebrew, and Mandarin Chinese, taking care to equate the level of difficulty of items across languages. The BNT was developed in New England and designed for American English speakers and contains items that either have no equivalent word or different frequencies of usage in other languages. The MINT is sensitive to naming impairment in AD.20
Word fluency is measured with semantic and letter word list generation tests. The former were part of UDSNB 2.0,whereas 2 letter generation tasks were added (“F” and “L”) for UDSNB 3.0. Each task requires 60 seconds and correct items are totaled. Note is made of errors and rule violations.
Visuospatial Tests
The UDSNB 2.0 did not contain a visuospatial test. Visuospatial symptoms emerge in later stages of amnestic dementia due to AD but also may appear early in the clinical syndromes of posterior cortical atrophy and dementia associated with cortical Lewy body disease. The Benson complex figure39 was added as a test of constructional ability (Copy condition). Figural elements are scored for presence and placement. Reproduction is tested after a delay to measure retentive memory (see the Episodic Memory section). Comparison between patients with clinical dementia of the Alzheimer type and frontotemporal dementia showed distinctive profiles of performance and associations with frontal and parietal cortical atrophy regions in the groups.39,41
Immediate Attention, Working Memory, Executive Attention Tests
Immediate attention span is commonly tested with Digit Span.18 For studies requiring multiple forms to reduce practice effects, a series of number sets was randomly generated to provide alternatives to the digit span test (Joel Kramer lab, personal oral communication). The number spans for the UDS task were randomly generated with the restriction that no digit would be adjacent to a digit that was one higher or one lower (eg, a “7” would not be succeeded or preceded by a 6 or 8). Every attempt was also made to exclude sequences that contained area codes. The number span is the longest list recalled. The total number of trials administered up to failure on 2 trials at 1 length is also recorded. Backward span is a measure of working memory. The trail making tests were retained from the UDSNB 2.0 to measure processing speed (part A) and executive attention (part B).
Study Sample
This report is based on analyses of UDS data submitted to NACC by the ADCs between March 15, 2015 and November 30, 2016. The sample was restricted to individuals who received the UDSNB 3.0 and at that visit had a clinical diagnosis of NC and a global CDR score of 0. If a participant had received UDSNB 3.0 more than once, data were included from only the first administration. Although some participants’ scores on the UDSNB 3.0 seemed to be outside the range of normal scores (eg, MoCA score of 9), we chose not to remove any participants from the descriptive analyses because normalcy was not defined by the tests. Therefore, we describe the full range of scores in those with a clinical diagnosis of NC and a global CDR=0.
We developed a calculator for the UDSNB 3.0 tests based on previously published methods used to produce the calculator for UDSNB 2.0 tests.6 Although our descriptive analyses focused on all participants meeting our eligibility criteria, for the normative calculator, we excluded a handful of participants who performed 5 SDs outside of the mean on any particular test to improve the distribution of residuals and better satisfy model assumptions.
RESULTS
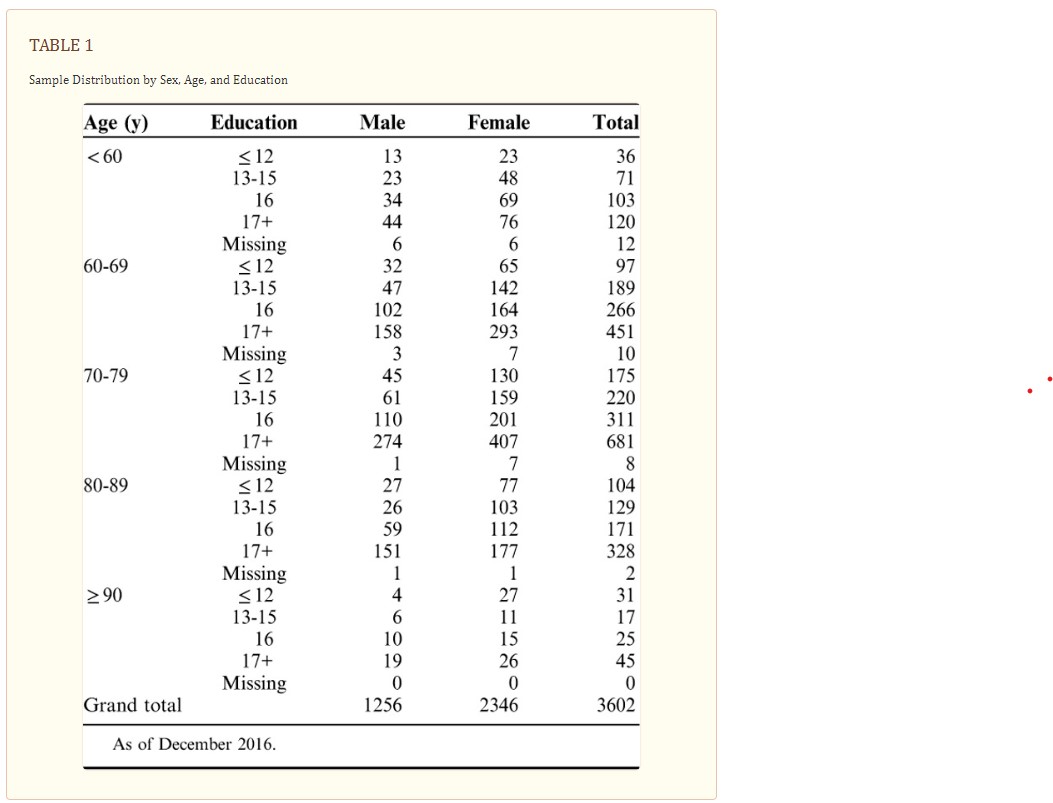
The sample included 3602 cognitively normal participants over age 60 receiving the UDSNB 3.0 (Table (Table1).1). The majority of the sample (65%) were women and were between 70 and 89 years of age (67%) and highly educated (69%). These analyses did not divide the sample by race, as most participants in the sample were white (83%), with an additional 14% African American, and 3% other race, reflecting the overall distribution of these groups within the ADCs receiving the UDS.
Means, 25th, 50th, and 75th percentile, and score ranges for each test in the overall sample are reported in Table Table2.2. Histograms demonstrate whether the distribution of test scores were approximately normal (Fig. (Fig.1).1). Tests with an approximately normal distribution of scores included Craft Story immediate and delayed (paraphrase and verbatim), number span forward and backward (total correct trials and longest span), the letter list generation task (F-words and L-words), and the Benson complex figure recall. Scores on the MoCA, MINT, and copy condition of the Benson complex figure copy were highly skewed due to ceiling effects. However, the MoCA seems to be less affected by ceiling effects than the MMSE.2
TABLE 2
Summary Statistics for Clinically Cognitively Normal UDS Participants
Histograms showing score distributions for each measure on the UDSNB 3.0. From these graphs, many of the measures have a normal or near normal distribution, with the exception of the MoCA total score, the score for the copy of the Benson complex figure, and the total score for the MINT. Immed. indicates immediate; MINT, multilingual naming test; MoCA, Montreal Cognitive Assessment; Paraph., paraphrase.
Table3 shows the means and SDs by each measure across the 5 age groups, and Table4 shows means and SDs for the 4 education groups. In the multivariable regression analyses (Table5), women performed statistically significantly (P<0.01) better than men on the Craft story immediate and delayed, verbal fluency phonemic test, and vegetables list generation, but worse on the Benson copy figure recall, number span forward, and MINT (Table5).. Women and men performed similarly, without statistically significant differences, on the Benson complex figure copy, number span backward, animal list generation, and trail making parts A and B. Increasing age was associated with worse scores and increasing years of education was associated with better scores on all of the tests (P<0.01).
TABLE 3
Mean Neuropsychological Test Scores by Age Group
TABLE 4
Mean Neuropsychological Test Scores by Education Group
TABLE 5
Multivariable Linear Regression Coefficients and 95% CIs for Sex, Age, and Education
For the data to be useful in characterizing research participants, a calculator was created to indicate the level of performance on each measure. The calculator uses the intercepts, regression coefficients, and root mean square errors resulting from the regression analyses described above to calculate unadjusted and adjusted Z-scores for individuals of a particular sex, age, and/or education level. The root mean square error is the square root of the average squared differences between the observed score and the predicted score, which we substitute as an estimate for a population SD. The adjusted Z-scores are calculated for each test adjusting for a single demographic characteristic (ie, sex, age, or education) and adjusting for all 3 of these demographics. One can enter an individual’s demographics and raw test scores, and the calculator uses the resulting Z-scores to calculate percentile estimates that indicate the individual’s level of impairment on any given test (eg, low average, or severely impaired). Two new variables were also added to this calculator to improve the precision of percentile estimates for trail making part A and part B. These 2 tests are terminated if the subjects cannot complete within a specified time length (150 s and 300 s for A and B, respectively), resulting in the same score regardless of how many lines are correctly connected. We added connections-per-second (correct lines connected divided by the time to completion) for both Part A and B. These 2 new variables provide more accurate Z-scores and percentiles for the trail making tests.
DISCUSSION
The current revision of the neuropsychological battery provides an updated set of tests, targeting predominantly the symptoms of the most typical, amnestic, presentation of AD. The tests are nonproprietary and have the potential to increase sensitivity over former measures to very early symptoms of cognitive decline in older individuals with different levels of education. The new measures are similar to the old measures but have also enriched the standard data collection with novel scores to enhance available data using a relatively brief battery. The normative calculator provides a convenient tool to characterize the level of performance on the measures of the UDSNB 3.0 battery. The calculator and the battery are available online (www.alz.washington.edu/WEB/npsych_means.html), (www.alz.washington.edu/NONMEMBER/UDS/DOCS/VER3/UDS3_npsych_worksheets_C2.pdf).