
This post is about the use of exercise oximetry with three clinically useful walking tests:
- 6 Minute Walking Test
- Incremental Shuttle Walk test (ISWT)
- Endurance Shuttle Walk test (ESWT)
The following is from Resource (1), How to carry out a field
walking test in chronic respiratory disease below:
Summary
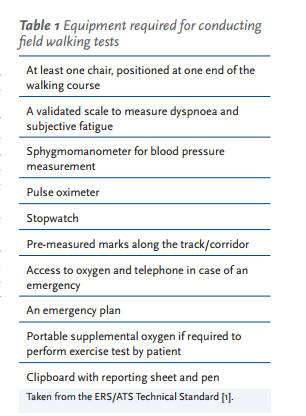
The European Respiratory Society (ERS) and American Thoracic Society (ATS) have recently published a Technical Standard which documents the standard operating procedures for the 6-min walk test (6MWT), incremental shuttle walk test (ISWT) and endurance shuttle walk test (ESWT). The Technical Standard shows that all three tests are valid and reliable measures of functional exercise capacity in people with chronic respiratory disease and makes recommendations for standardising their performance. Key findings and recommendations of the Technical Standard include:
● The 6MWT, ISWT and ESWT are strenuous tests which elicit cardiorespiratory responses that are similar to those observed during a maximal incremental exercise test. As a result, the contraindications and precautions for field walking tests should be consistent with those used for a laboratory-based incremental exercise test.
● There is strong evidence of a learning effect for the 6MWT and ISWT. Two tests should be performed when the 6MWT or ISWT are used to measure change over time.
● The 6MWT, ISWT and ESWT are responsive to treatment effects in people with chronic respiratory disease, particularly for rehabilitation. ● The 6MWT is very sensitive to variations in methodology, including use of encouragement, provision of supplemental oxygen, changes in track layout and length, and use of wheeled walkers. These factors should be documented and held constant on repeat testing.
● The lowest SpO2 recorded during a 6MWT is an important marker of disease severity and prognosis. Continuous pulse oximetry is recommended during the 6MWT, to ensure that the lowest SpO2 is recorded.
● In adults with chronic respiratory disease, a change in 6-min walk distance of 30 m or more indicates a clinically significant change has occurred.
I think that the Massimo Fingertip Pulse Oximeter With Bluetooth might be quite suitable for walking tests. I have not yet used it but plan to.
There should also , at minimum, an automated external defibrillator in the test room. If a physician is monitoring the test, it might be a good idea to have a monitor-defibrillator and the recommended Advanced Cardiac Life Support drugs.

Purpose of the tests
Field walking tests may be performed to identify the patient’s exercise capacity (peak exercise capacity, functional exercise capacity or endurance), factors limiting exercise performance (dyspnoea, subjective fatigue, musculoskeletal limitations) and often their response to an intervention. The field tests can also be used to identify a threshold to predict survival and the likelihood of a hospital readmission, with a more extensive body of evidence reporting use of 6MWD rather than ISWT or ESWT for this purpose [2]. Prescription of exercise intensity for pulmonary rehabilitation may also be a consideration. The 6MWT and the ISWT/ESWT have been reported in all of these circumstances [2]
Patient assessment
Field walking tests have a good safety profile,
with few adverse events reported in the
literature [2]. However, in recent years, it has
become clear that the 6MWT, ISWT and ESWT
are strenuous tests for people with moderate
to severe chronic lung disease, eliciting cardiorespiratory
responses that are similar to those
seen on a maximal, incremental exercise test
[2]. Because of this, the Technical Standard
recommends that the absolute and relative
contraindications for exercise testing should
be consistent with recommendations for maximal
exercise testing [35] (table 2). Patients with
any of these findings should be referred to the
physician ordering or supervising the test for
individual clinical assessment and a decision
about whether the test should go ahead.Use of oxygen
If a patient is on long-term oxygen therapy, oxygen should be given at their standard flow rate or as directed by a physician or a protocol. For any test where the outcome is distance, oxygen flow rate should be held constant throughout the test. If the purpose of the exercise test is to compare distance walked between tests, any subsequent test should be performed using the same oxygen conditions, in order to make a valid comparison between testing occasions. If the flow rate must be increased for subsequent visits due to worsening gas exchange, this should be noted on the worksheet and considered during interpretation of any changes in performance.
Measurements
Patients should rest in a chair, located near the starting position, before the test starts. Check for absolute and relative contraindications prior to test commencement (table 2). The following measurements should be obtained at rest: ● SpO2 and heart rate from pulse oximetry ● Baseline dyspnoea and fatigue using a reproducible scale (e.g. Borg scale) ● Systemic blood pressure, if not recently documented.
Immediately prior to the test
The assessor should provide standardised instructions, either verbally for the 6MWT (table 3) or from the ISWT or ESWT audio recording. Position the patient at the starting line. For the 6MWT, start the timer as soon as the patient starts to walk. The recorded instructions of the ISWT and ESWT will prompt the patient to start.
Immediately on test cessation
Record SpO2 and heart rate from the oximeter; ask the patient to rate their dyspnoea and subjective fatigue on the standardised scale. It is important to understand the patient’s perception of limitations to their performance, so patients should be asked why they could not walk any further. It is common for patients to report either dyspnoea or leg fatigue as the primary factor limiting their performance on the test
Reasons for the assessor to stop an exercise test
In some patients, profound desaturation (SpO2 <80%) may occur during a field walking test. Use of a 6MWT protocol where the test is stopped if SpO2 falls to <80% is associated
with an extremely low rate of adverse events [37]; this has not been reported for the ISWT or ESWT. Few data are available to determine the risk if the test is not stopped when SpO2 falls to <80%. Stopping the test when SpO2 falls to <80% is also consistent with the recommendations for incremental exercise testing [35]. If SpO2 recovers to ≥85% during the 6MWT, the patient may be asked to recommence walking.Other reasons for stopping the test include chest pain, intolerable dyspnoea, leg cramps, staggering, diaphoresis and a pale or ashen appearance. If a test is stopped for any of these reasons, the patient should sit or lie supine as appropriate. The following should be obtained based on the judgment of the assessor: blood pressure, pulse rate, SpO2, and a physician evaluation. Oxygen should be administered as appropriate.
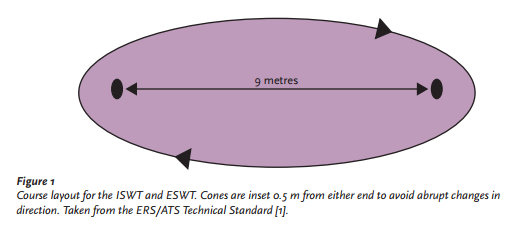
The course layout of the Incremental Shuttle Walk Test (ISWT) and of the the Endurance Shuttle Walk Test (ESWT) are the same.
The incremental and endurance shuttle walking tests
The ISWT is an externally paced maximal exercise test where the speed of walking increases with each level, controlled by a series of pre-recorded signals. The test continues until the participant can no longer continue or cannot keep up with the required pace. The maximum duration of the test is 20 min. The ISWT is a valid measure of a cardiopulmonary exercise capacity in COPD and provokes a similar physiological response to a cardiopulmonary exercise test [2]. A lower ISWT predicts poor survival and increase risk of hospital re-admission in people with COPD [25–27]; however, there are few data on its use in patients with chronic respiratory disorders other than COPD. The ISWT is a reliable test, but there is evidence of a learning effect on the second test in the range of 20–25 m [2]. This is large enough to be clinically important when evaluating change over time. As a result, it is recommended that two ISWTs are performed and the best distance recorded [1].
The endurance shuttle walking test (ESWT) is a derivative of the ISWT, where patients walk for as long as possible at a predetermined percentage of maximum walking performance as assessed by the ISWT, frequently in the range of 70–85% [28]. To set the speed for the ESWT, the ISWT must have been determined previously. One test is sufficient to obtain a reliable measure.
Three papers have described reference values for the ISWT, two from South America [32, 33] and one from the UK [34]. There are no reference equations for the ESWT.
There are detailed instructions in Resource (1) on how to conduct the ISWT and the ESWT on pages 135 – 137 (pp 8 – 11 of the PDF)
There are also detailed instructions in Resource (1) on how to conduct the 6 Minute Walk Test on pages 134 and 135 (pp 7 + 8) of the PDF)
The course layout of the 6 Minute Walk Test (6MWT) is different from the ISWT and the ESWT:
The 6 Minute Walk Test
The 6MWT should be performed along a flat, straight course with a hard surface with little pedestrian traffic. It is recommended that the walking course be ≥30 m in length, to be consistent with the courses on which reference equations have been generated [2]. The ends of the course should be marked so that they are easily visible to patients.
Resources:
(1) How to carry out a field walking test in chronic respiratory disease [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Breathe (Sheff). 2015 Jun;11(2):128-39. doi: 10.1183/20734735.021314.
(2) An official European Respiratory Society/American Thoracic Society technical standard: field walking tests in chronic respiratory disease [PubMed Abstract] [Full Text HTML] [Full Text PDF].Eur Respir J. 2014 Dec;44(6):1428-46. doi: 10.1183/09031936.00150314. Epub 2014 Oct 30.
(3) An official systematic review of the European Respiratory Society/American Thoracic Society: measurement properties of field walking tests in chronic respiratory disease [PubMed Abstract] [Full Text HTML] [Full Text PDF]. Eur Respir J. 2014 Dec;44(6):1447-78. doi: 10.1183/09031936.00150414. Epub 2014 Oct 30.
(4) Reference Standards For The 6 Minute Walk Test And Other Resources On Exercise Assessment Posted on July 19, 2018 by Tom Wade MD



