Today, I review, link to, and excerpt from Stroke‘s Guidelines in Action: Getting to the (Large) Core of the (T)Issue [No abstract available] [Full-Text HTML] [Full-Text PDF]. Stroke. 2026 Jan 26. doi: 10.1161/STROKEAHA.125.053822. Online ahead of print.
All that follows is from the above resource.
A 65-year-old man with a history of hypertension and atrial fibrillation off anticoagulation presented to the emergency room via emergency medical services following a series of falls at home and slurred speech. He had been feeling unwell the days leading up to the presentation, but was neurologically at baseline the night prior. That evening, he had several falls before getting to bed. The following morning, he called his sister to report the falls, and she noted slurring of his speech and called emergency medical services.
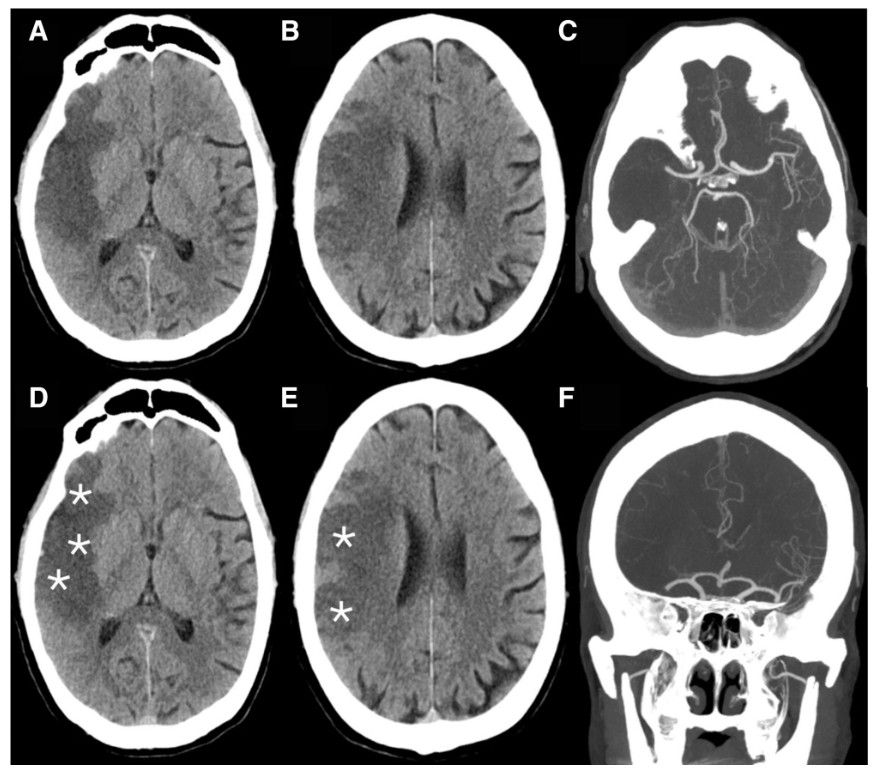
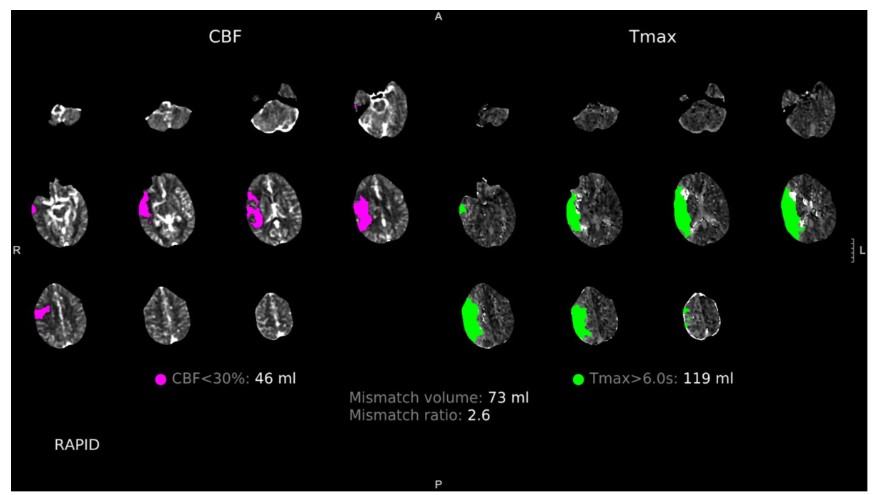
Before hospital arrival, emergency medical services activated a prehospital stroke alert to ready the appropriate teams. On arrival to the emergency room at ≈12.5 hours from last known well, he was noted to have a right middle cerebral artery syndrome with a National Institutes of Health Stroke Scale score of 9: right gaze preference (1), left facial droop (2), mild drift in the left arm (1) and leg (1), left-sided sensory deficit (1), left-sided extinction/inattention (2), and mild dysarthria (1). Computed tomography (CT) of the head noted early ischemic changes in the right middle cerebral artery territory with an Alberta Stroke Program Early Computed Tomography Score (ASPECTS) of 5 (Figure 1). CT angiography of the head and neck revealed a distal M1 segment of the right middle cerebral artery large vessel occlusion (Figure 1). CT perfusion imaging of the head estimated 46 mL of core infarction and 119 mL of penumbra (Figure 2). He was taken for endovascular thrombectomy (EVT), which achieved Thrombolysis in Cerebral Infarction 2b reperfusion.
Figure 1. A man with a history of atrial fibrillation off anticoagulation and hypertension presented with an acute right middle cerebral artery (MCA) stroke. A and B, Computed tomography (CT) of the head demonstrates early ischemic change in the right MCA territory. D and E, CT of the head reveals Alberta Stroke Program Early Computed Tomography Score (ASPECTS) of 5 with asterisks identifying regions exhibiting early ischemic change. C (axial) and F (coronal), Computed tomography angiography (CTA) of the head and neck revealed occlusion of the distal M1 segment of the right MCA.
Figure 2. A man with a history of atrial fibrillation off anticoagulation and hypertension presented with an acute right middle cerebral artery (MCA) stroke. Computed tomography perfusion (CTP) of the brain estimates 46 mL of core infarction as highlighted in pink on the cerebral blood flow (CBF) map, and 119 mL of penumbra as highlighted in green on the time-to-maximum of the tissue residue function (Tmax) map.
On hospital day 2, his National Institutes of Health Stroke Scale score had improved to 4: slight left facial droop (1), left-sided sensory deficit (1), left-sided extinction/inattention (1), and mild dysarthria (1). Magnetic resonance imaging of the brain demonstrated acute ischemia corresponding to the regions of early ischemic change noted on CT. His discharge examination noted a National Institutes of Health Stroke Scale score of 2, scoring for left-sided nasolabial fold flattening (1) and mild dysarthria (1). His left-sided neglect, weakness, sensory deficit, and right-sided gaze preference had resolved by that time, and his modified Rankin Scale score was 1. At the 90-day follow-up, he reported being returned to baseline with a modified Rankin Scale score of 0.
DISCUSSION
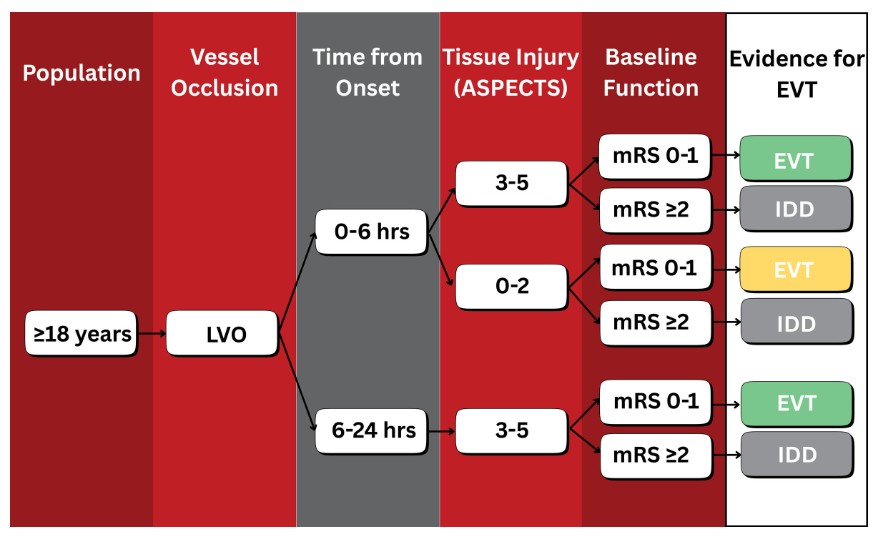
Here, we present a clinical case to highlight how to implement the 2026 Guideline for the Early Management of Patients With Acute Ischemic Stroke (AIS) for patients with large core ischemic stroke. This case clearly illustrates the guideline recommendation (class 1, level A evidence) that for “selected patients with AIS from anterior circulation proximal large vessel occlusion of the internal carotid artery or M1, presenting between 6 and 24 hours from onset of symptoms, with age <80 years, National Institutes of Health Stroke Scale score ≥6, prestroke modified Rankin Scale score 0 to 1, ASPECTS 3 to 5, and without significant mass effect on imaging, EVT is recommended to improve functional clinical outcomes and reduce mortality.”1A large core ischemic infarct is typically defined by a cerebral infarct volume of >50 to 70 mL or by an ASPECTS score of ≤5. Approximately 8% to 25% of patients with large vessel occlusion have a large core infarct. Historically, patients meeting these definitions of large core infarction were excluded or underrepresented in the first generation of randomized controlled trials that proved the efficacy of EVT for acute ischemic stroke. The rationale was partially due to the perceived risk of postreperfusion hemorrhage and edema within the core infarct. Additionally, given the association between larger core infarcts and worse functional outcomes, there was concern that including such patients may reduce the net treatment benefit from EVT. Yet, observational studies suggested that EVT for large core infarct may be associated with improved functional outcomes compared with best medical treatment.2The new 2026 American Heart Association (AHA)/American Stroke Association (ASA) AIS Guidelines have now been released in the context of 6 randomized controlled trials published between 2022 to 2024 that expanded the historical EVT trial selection criteria and proved the efficacy of EVT for large core ischemic stroke. Published in April 2022, RESCUE-Japan LIMIT (Recovery by Endovascular Salvage for Cerebral Ultra-Acute Embolism Japan Large Ischemic Core Trial) was a multicenter randomized clinical trial in Japan including patients with large vessel occlusion and ASPECTS of 3 to 5, which found that patients who underwent EVT had better functional outcomes than those receiving best medical treatment.3 In February 2023, the SELECT-2 (Randomized Controlled Trial to Optimize Patient’s Selection for Endovascular Treatment in Acute Ischemic Stroke) and ANGEL-ASPECT (Study of Endovascular Therapy in Acute Anterior Circulation Large Vessel Occlusive Patients With a Large Infarct Core) trials reported similar evidence of benefit in similar populations of large core patients who underwent EVT.4,5 TESLA (Thrombectomy for Emergent Salvage of Large Anterior Circulation Ischemic Stroke) included patients with last known well up to 24 hours with ASPECTS of 2 to 5, but found no significant difference in outcomes between the EVT and medical management arms.6 The TENSION study (Efficacy and Safety of Thrombectomy in Stroke With Extended Lesion and Extended Time Window)7 and in May 2024, the LASTE trial (Large Stroke Therapy Evaluation; which included patients with ASPECTS ≤5, with the majority having values ≤2),8 both found better functional outcomes and lower mortality in patients receiving EVT versus those who received best medical treatment alone.While it is now clear that EVT for large core ischemic infarct improves outcomes, the large core randomized controlled trials had varied inclusion/exclusion criteria with respect to treatment time window, imaging modality used (CT versus magnetic resonance imaging ASPECTS versus CT perfusion imaging), and size/severity of large core infarction.9 This heterogeneity may lead to challenges when applying the results of these trials clinically. For example, our patient had a CT ASPECTS of 5, yet the CT perfusion estimated 46 cm3 of core infarct. How should clinicians proceed when there is disagreement between ASPECTS and CT perfusion volumetric scoring systems? The 2026 AHA/ASA AIS Guidelines provide a useful algorithm for the management of AIS eligibility for EVT (reproduced in Figure 3, highlighting the large core recommendations). This algorithm utilizes ASPECTS scores to define EVT eligibility. Yet, the guideline notes an important knowledge gap and future area for research is to evaluate the predictive value of specific volumes of infarct and degrees of CT hypodensity/diffusion weighted imaging restriction to further refine EVT selection for patients with ASPECTS <6.1Figure 3. Algorithm for management of acute ischemic stroke (AIS) eligibility for endovascular thrombectomy (EVT) for large core infarct. Green = Class 1 (strong) recommendation. Yellow = Class 2a (moderate) recommendation. ASPECTS indicates Alberta Stroke Program Early Computed Tomography Score; IDD, insufficient data to determine; LVO, large vessel occlusion; and mRS, modified Rankin Scale. Adapted from Prabhakaran et al1 with permission. Copyright ©2026, the American Heart Association Inc.Take-Home Points
• For patients with large core ischemic infarct meeting guideline criteria, the 2026 Acute Ischemic Stroke Guidelines recommend endovascular thrombectomy to improve functional clinical outcomes and reduce mortality (level 1, class A evidence).• There was significant heterogeneity in the inclusion/exclusion criteria for the 6 large core endovascular thrombectomy randomized controlled trials, which has led to knowledge gaps and areas for future research.• In light of the large core randomized trials and 2026 Guidelines expanding the indication for endovascular thrombectomy, acute stroke systems of care will need to adapt to ensure the growing demands for endovascular thrombectomy are met.The new AIS guideline also highlights that while large core patients receiving EVT more than doubled their rate of functional independence compared with patients receiving best medical treatment alone, the proportion of patients achieving functional independence was substantially lower than that seen in earlier EVT trials (19.5% versus ≈50%). This reflects the greater severity of illness in this population and underscores the need for frank and careful discussions with the patient and family about the risk/benefit calculus of intervention.1 Nevertheless, these positive large core EVT trials represent a major advance in acute stroke care and will markedly expand the number of potentially eligible patients.10 Acute stroke systems of care will need to respond accordingly to ensure the growing demand for EVT is met.References
1. Prabhakaran S, Gonzalez NR, Zachrison KS, Adeoye O, Alexandrov AW, Ansari SA, Chapman S, Czap AL, Dumitrascu OM, Ishida K, et al. 2026 Guideline for the early management of patients with acute ischemic stroke: a guideline from the American Heart Association/American Stroke Association. Stroke. 2026;57:exxx–xxxx. doi: 10.1161/STR.00000000000005132. Kaesmacher J, Chaloulos-Iakovidis P, Panos L, Mordasini P, Michel P, Hajdu SD, Ribo M, Requena M, Maegerlein C, Friedrich B, et al. Mechanical thrombectomy in ischemic stroke patients with Alberta Stroke Program Early Computed Tomography Score 0-5. Stroke. 2019;50:880–888. doi: 10.1161/STROKEAHA.118.0234653. Yoshimura S, Sakai N, Yamagami H, Uchida K, Beppu M, Toyoda K, Matsumaru Y, Matsumoto Y, Kimura K, Takeuchi M, et al. Endovascular therapy for acute stroke with a large ischemic region. N Engl J Med. 2022;386:1303–1313. doi: 10.1056/NEJMoa21181914. Sarraj A, Hassan AE, Abraham MG, Ortega-Gutierrez S, Kasner SE, Hussain MS, Chen M, Blackburn S, Sitton CW, Churilov L, et al; SELECT2 Investigators. Trial of endovascular thrombectomy for large ischemic strokes. N Engl J Med. 2023;388:1259–1271. doi: 10.1056/NEJMoa22144035. Huo X, Ma G, Tong X, Zhang X, Pan Y, Nguyen TN, Yuan G, Han H, Chen W, Wei M, et al;. ANGEL-ASPECT Investigators. Trial of endovascular therapy for acute ischemic stroke with large infarct. N Engl J Med. 2023;388:1272–1283. doi: 10.1056/NEJMoa22133796. Writing Committee for the TESLA Investigators; Yoo AJ, Zaidat OO, Sheth SA, Rai AT, Ortega-Gutierrez S, Given CA, Zaidi SF, Grandhi R, Cuellar H, Mokin M; TESLA Investigators. Thrombectomy for stroke with large infarct on noncontrast CT: the TESLA randomized clinical trial. JAMA. 2024;332:1355–1366. doi: 10.1001/jama.2024.139337. Bendszus M, Fiehler J, Subtil F, Bonekamp S, Aamodt AH, Fuentes B, Gizewski ER, Hill MD, Krajina A, Pierot L, et al; TENSION Investigators. Endovascular thrombectomy for acute ischaemic stroke with established large infarct: multicentre, open-label, randomised trial. Lancet. 2023;402:1753–1763. doi: 10.1016/S0140-6736(23)02032-98. Costalat V, Jovin TG, Albucher JF, Cognard C, Henon H, Nouri N, Gory B, Richard S, Marnat G, Sibon I, et al; LASTE Trial Investigators. Trial of thrombectomy for stroke with a large infarct of unrestricted size. N Engl J Med. 2024;390:1677–1689. doi: 10.1056/NEJMoa23140639. Liu C, Abdalkader M, Sang H, Sarraj A, Campbell BCV, Miao Z, Huo X, Yoo AJ, Zaidat OO, Thomalla G, et al. Endovascular thrombectomy for large ischemic core stroke: a systematic review and meta-analysis of randomized controlled trials. Neurology. 2025;104:e213443. doi: 10.1212/WNL.000000000021344310. Mistry EA, Khoury JC, Kleindorfer DO, Kissela BM, Alwell KS, Jasne AS, Ferioli S, De Los Rios La Rosa F, Coleman E, Demel SL, et al. Projections of endovascular therapy-eligible patients with stroke for the US population. Stroke. 2024;55:2011–2019. doi: 10.1161/STROKEAHA.123.045766