In this post, I link to and excerpt from Acute-on-chronic liver failure: an update [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Gut. 2017 Mar;66(3):541-553. doi: 10.1136/gutjnl-2016-312670. Epub 2017 Jan 4.
All that follows is from the above resource.
See editorial “Acute-on-chronic liver failure—old concepts made clearer” in Transl Gastroenterol Hepatol, volume 2, 111.
Abstract
Acute-on-chronic liver failure (ACLF) is a syndrome characterised by acute decompensation of chronic liver disease associated with organ failures and high short-term mortality. Alcohol and chronic viral hepatitis are the most common underlying liver diseases. Up to 40%–50% of the cases of ACLF have no identifiable trigger; in the remaining patients, sepsis, active alcoholism and relapse of chronic viral hepatitis are the most common reported precipitating factors. An excessive systemic inflammatory response seems to play a crucial role in the development of ACLF. Using a liver-adapted sequential organ assessment failure score, it is possible to triage and prognosticate the outcome of patients with ACLF. The course of ACLF is dynamic and changes over the course of hospital admission. Most of the patients will have a clear prognosis between day 3 and 7 of hospital admission and clinical decisions such as evaluation for liver transplant or discussion over goals of care could be tailored using clinical scores. Bioartificial liver support systems, granulocyte-colony stimulating factors or stem-cell transplant are in the horizon of medical care of this patient population; however, data are too premature to implement them as standard of care.
Keywords: LIVER CIRRHOSIS, LIVER FAILURE
Introduction
Cirrhosis is a pathological diagnosis characterised by diffuse fibrosis, severe disruption of the intrahepatic arterial and venous flow, portal hypertension and, ultimately, liver failure.1 Traditionally, cirrhosis has been dichotomised in compensated and decompensated, and the transition to decompensated cirrhosis happens when any of the following hallmarks occurs: presence of ascites, variceal haemorrhage and/or hepatic encephalopathy (HE).2 Once cirrhosis transitions from the compensated to the decompensated stage, it is associated with short-term survival (3–5 years) and evaluation for liver transplant is recommended in the absence of contraindications. If cirrhosis is mediated by a treatable cause (eg, chronic viral hepatitis, ongoing alcohol consumption, obesity, etc), then patients may have transition from a decompensated to a compensated phase.
The concept of acute-on-chronic liver failure (ACLF) has been widely used in critical care hepatology to study patients who underwent artificial support therapies as a bridge to liver transplantation (LT).3 . . . The current narrative review will provide insights on the current understanding of ACLF with emphasis on established definitions, epidemiology, pathophysiology and treatment/management options.
Heterogeneity of definitions
ACLF is a syndrome characterised by acute and severe hepatic abnormalities resulting from different types of insults, in patients with underlying chronic liver disease or cirrhosis but, in contrast to decompensated cirrhosis, has a high short-term mortality, mimicking the prognosis of acute liver failure.
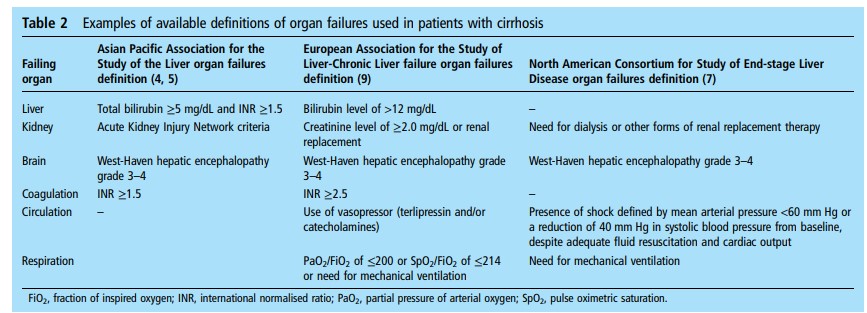
*West-Haven hepatic encephalopathy score-Hepatic Encephalopathy: Definition, Clinical Grading and Diagnostic Principles [Full-Text HTML]. Drugs. 2019; 79(Suppl 1): 5–9.
Published online 2019 Jan 31. doi: 10.1007/s40265-018-1018-z
Underlying chronic liver disease and triggering factors
Prevalence of ACLF
The variety of definitions makes quite difficult to predict what
would be an accurate proportion of patients with cirrhosis who
would meet criteria for ACLF. Nevertheless, based on hospital
registries it is reasonable to estimate that ACLF is present in
between 24% and 40% of patients with cirrhosis admitted to
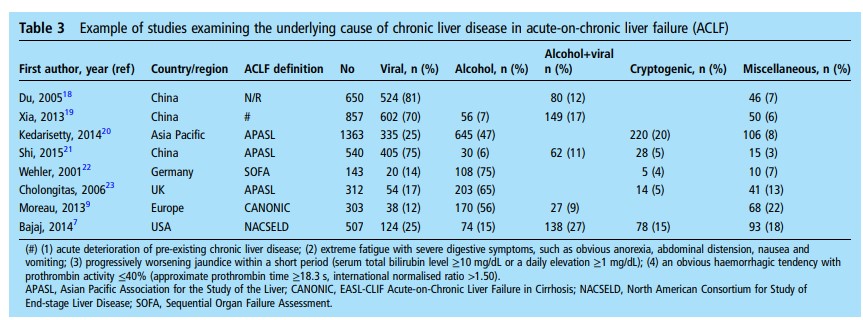
the hospital.7 9 12–15Aetiology of chronic liver disease in ACLF
Adapted from Abbas and Shazi,16 table 3 summarises selected
original publications examining the underlying chronic liver
disease in populations with ACLF.
Viral hepatitis, alcohol or a combination of both are the predominant causes of underlying chronic liver disease in ACLF in the world. The change in dietary patterns and lifestyle will likely lead to a shift on the ACLF predisposing disease and, as other areas in hepatology, it would not be surprising if non-alcoholic steatohepatitis took the lead in years to come.17
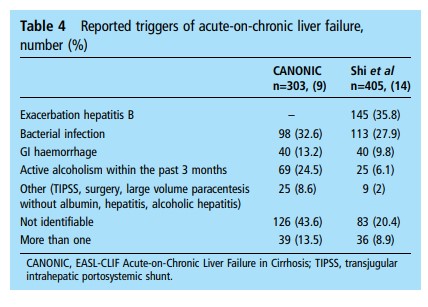
Triggers of decompensation in ACLF
The prevalence of potential triggers also varies by the area of
the world. For example, in the CANONIC study, bacterial infections and alcoholism are the two major identifiable factors, compared with China, where relapse of hepatitis B was predominant followed by bacterial infections9 14 (table 4).Despite exhaustive examination, in 20%–45% of cases, the
trigger remains unknown.Organ failureIn the CANONIC study, the kidneys were the most common
affected organs (55.8% of patients), followed by the liver (43.6%
of patients), coagulation (27.7% of patients), the brain (24.1% of
patients), circulation (16.8% of patients) and the lungs (9.2% of
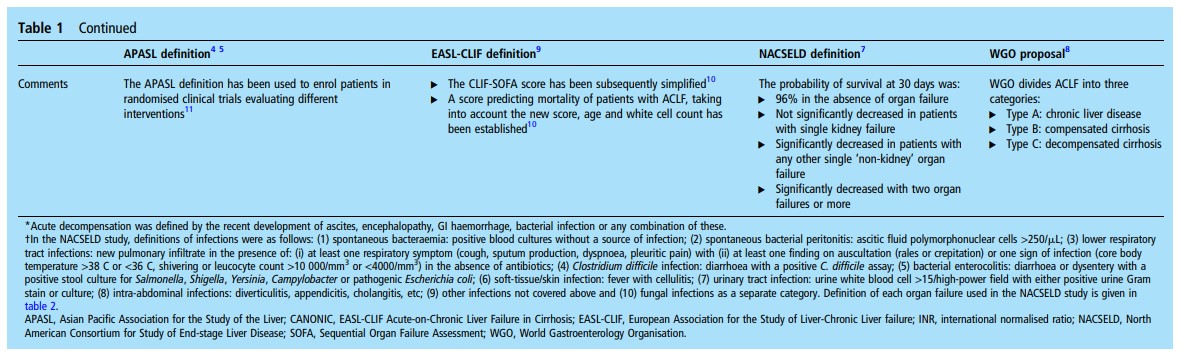
patients).9In the NACSELD study, 55.7% had grade III–IV HE,
17.6% developed shock, 15.1% required renal replacement
therapy and 15.8% required mechanical ventilation.7PATHOPHYSIOLOGY OF SYSTEMIC INFLAMMATION IN
ACLFSystemic inflammation is a hallmark of ACLF;9 24 white cell
count and plasma levels of C reactive protein (CRP) and
pro-inflammatory molecules such as interleukin (IL)-6, IL-1β,
IL-8 are higher in patients with ACLF than in those
without.25 26General principles of the inflammatory responseThe inflammatory response develops when inducers of inflammation are recognised by sensors that engage effectors of the response.27–29Inducers of inflammationInducers of inflammation are either exogenous or endogenous.27–29 Among exogenous inducers, only microbial inducers will be discussed because the others have been already
reviewed28 and are beyond the scope of ACLF.
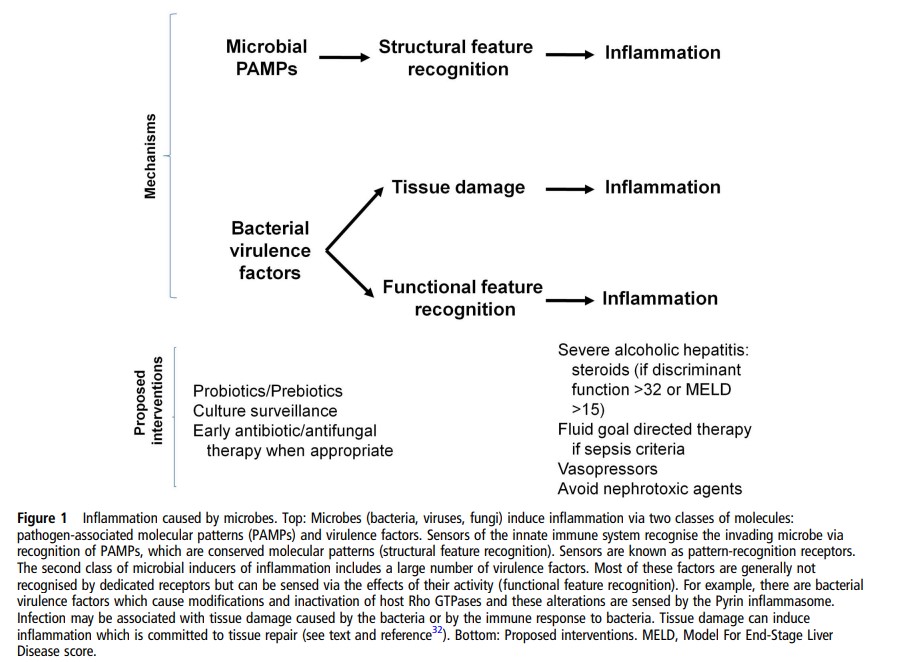
Microbial inducersBacterial inducersBacteria trigger inflammation by using two distinct classes of
molecules: pathogen-associated molecular patterns
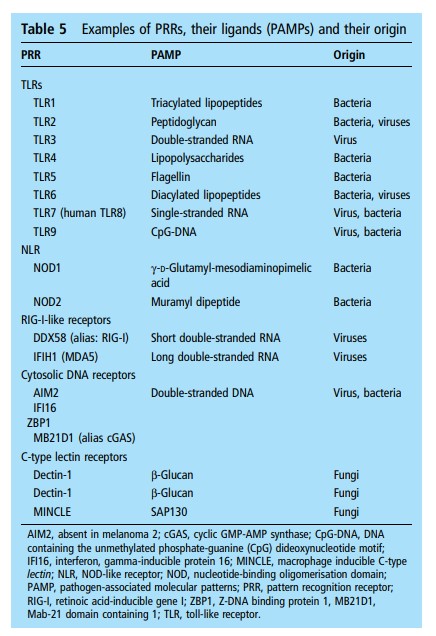
(PAMPs)27 29–31 and virulence factors.27–29 PAMPs are unique molecular signatures that are recognised via dedicated receptors called pattern-recognition receptors (PRRs), a process called structural feature recognition (figure 1) 32 (table 5).PRRs are expressed in innate immune cells and epithelial
cells.32 . . . PRR engagement by PAMPs stimulates intracellular signalling cascades that activate transcription factors, for example, nuclear factor-κB.30 31 PRR-activated transcription factors induce a broad variety of genes encoding molecules involved in inflammation such as cytokines, chemokines, among others.30 31Virulence factors represent the second class of bacterial inducers of inflammation.27–29 32 These factors are generally not recognised by dedicated receptors but detected through the
effects of their activity (a process called functional feature recognition) (figure 1).28 32 At the site of infection, the detection of the presence of the bacteria via the recognition of structural and functional bacterial features is thought to induce complementary responses aiming to eliminate the invading microbe.32Other microbesViruses or fungi are recognised by different PRRs (table 5). For
example, viral nucleic acids can be recognised by endosomal
TLRs, cytosolic receptors (RLRs or DNA sensors). Fungi
express PAMPs that are detected by C-type lectin receptors.
Like detection of bacterial PAMPs, that of viral or fungal
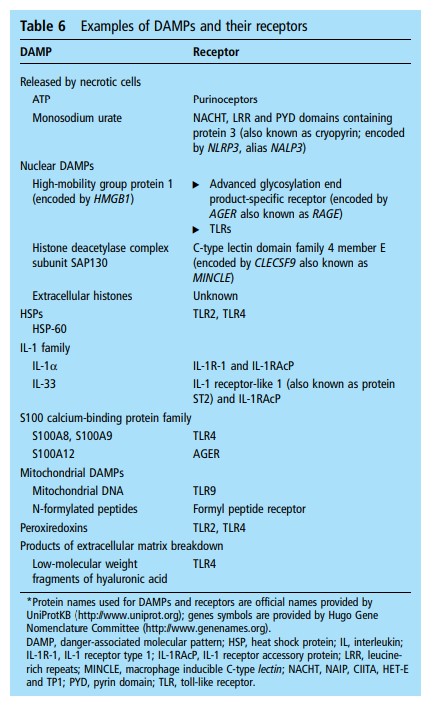
PAMPs can trigger inflammation (figure 1).Endogenous inducersEndogenous inducers are released by necrotic cells or as a result
of extracellular matrix breakdown.28 33 These endogenous inducers are called danger-associated molecular patterns (DAMPs)33 because they alert the host’s immune system about the presence of a serious tissue injury. DAMPs are recognised by receptors of the host (table 6) and this recognition induces sterile
inflammation.ACLF with identified inducers of inflammationSepsis-induced ACLFSystemic inflammation and the development of OFs are attributed to bacterial infection in approximately 30% of patients with ACLF.9 These patients have sepsis-induced ACLF. The most common infection causing sepsis-induced ACLF is spontaneous bacterial peritonitis (SBP).9 SBP is a paradigm in that it is often caused by Gram-negative bacteria that have migrated from the intestinal lumen to ascitic fluid via the systemic circulation.Severe alcoholic hepatitisSevere alcoholic hepatitis (SAH) represents approximately 25%
of the cases of ACLF.9 Severity is related to the development of
OFs.9 Systemic inflammation develops in patients with SAH and
correlates with the outcome suggesting a role of inflammation in the development of OFs.41 Systemic inflammation can be caused
by bacterial infection which is present in ∼30% of patients
admitted to the hospital for SAH.42 Excessive alcohol consumption is associated with intestinal dysbiosis and increased intestinal permeability, which favour translocation of viable bacteria.27 This may explain why SBP is the most common infection at admission of patients with SAH.42 However, systemic inflammation is also observed in patients with SAH without clinically detectable bacterial infection.9 41 In this context, the mechanisms explaining systemic inflammation are unclear.ACLF with no obvious triggerAbout 40%–50% of patients with ACLF have systemic inflammation for which there are no clinically identifiable triggers.9
DIAGNOSIS
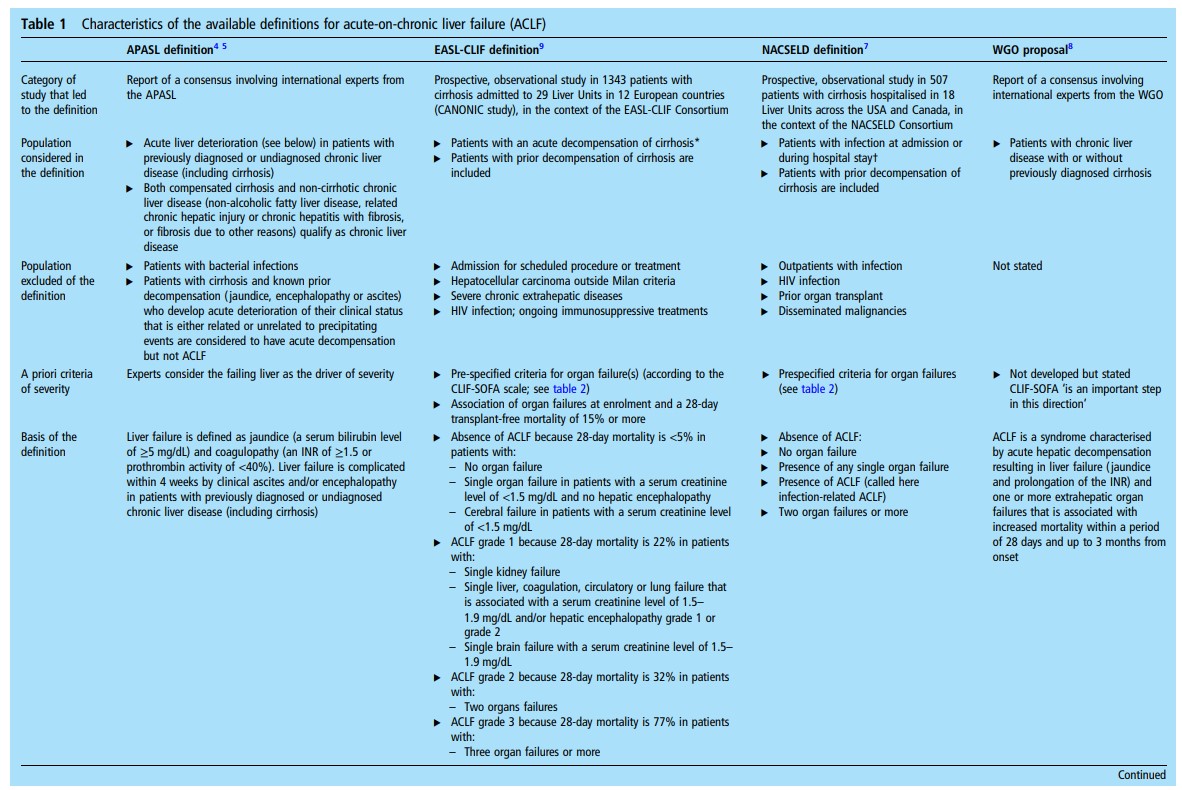
Among all operational definitions of ACLF (table 1), the definition and diagnostic criteria proposed by the EASL-CLIF
Consortium represent the first one based on large prospective
data including all patients with cirrhosis, regardless of the presence of infection, from a multicentre European prospective
cohort, the CANONIC study. According to this cohort, ACLF is
defined as acute decompensation (AD) of cirrhosis associated
with OF and high short-term mortality (28-day mortality
≥15%).9 The SOFA score was the model used for the diagnosis
of OF, as it is a widely used method in critically ill patients and
is superior to Model For End-Stage Liver Disease (MELD) score
in predicting prognosis in patients with AD of cirrhosis associated with OFs.9 50 Considering that the components of SOFA score (liver, kidney, brain, coagulation, circulation and lungs) do not take into account specific characteristics of patients with cirrhosis, the method used for the diagnosis of ACLF was a modified version of SOFA score, called CLIF-SOFA score. This was later simplified in a new version called CLIF Consortium Organ Failure score (CLIF-C OFs)10 (table 7).
On this background, diagnostic criteria of ACLF were established according to the presence, type and number of OFs.
Severity of ACLF was graded into different stages according to
the number of OFs on ACLF grade 1, grade 2 and grade 39
(table 1, under EASL-CLIF column) and mortality correlates
with ACLF severity (figure 2).It should be noted that ACLF may occur both in patients with
previously compensated or decompensated cirrhosis, and also in
patients with underlying chronic liver disease without cirrhosis.NATURAL HISTORY AND ASSESSMENT OF PROGNOSIS IN
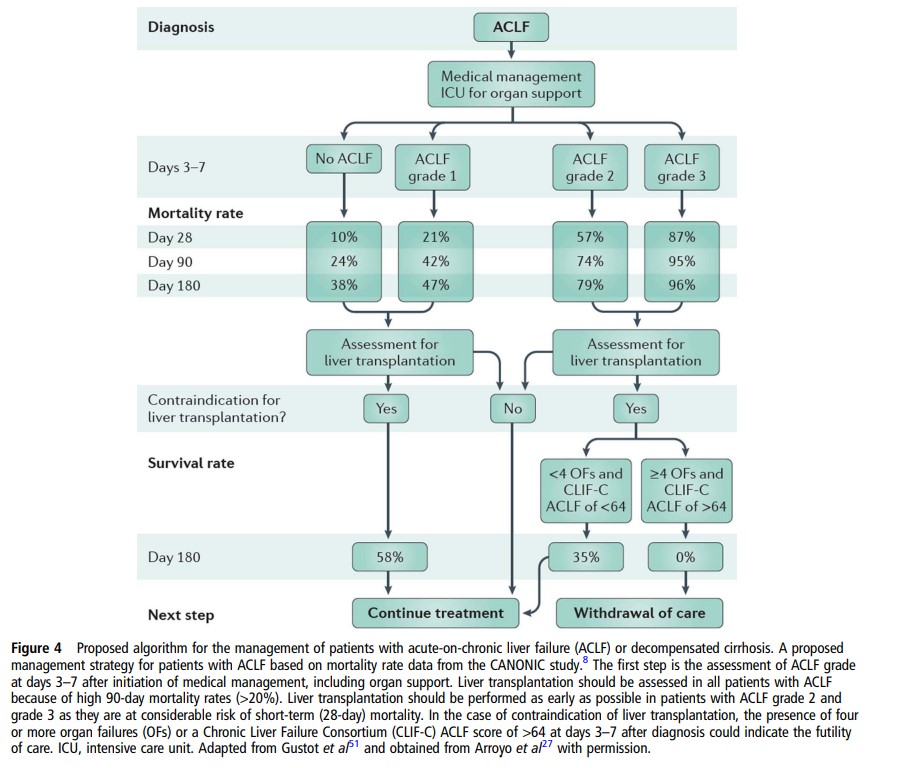
PATIENTS WITH ACLFACLF grade predicts mortality As described above, ACLF is associated with high short-term mortality. ACLF grade at diagnosis is associated with short-term prognosis, with patients with ACLF grade 3 showing the worst prognosis compared with that of patients with ACLF grade 1 and 2. Data from the CANONIC study showed overall 28-day mortality of 33% of all cases of ACLF, and specific 28-day mortality rates in patients with ACLF grade 1, 2 and 3 was 22%, 32% and 73%,respectively9 (figure 2).Therefore, it is very important to stratify patients according
to prognosis, in order to monitor treatment responsiveness,
determine emergency for transplantation, decide allocation in
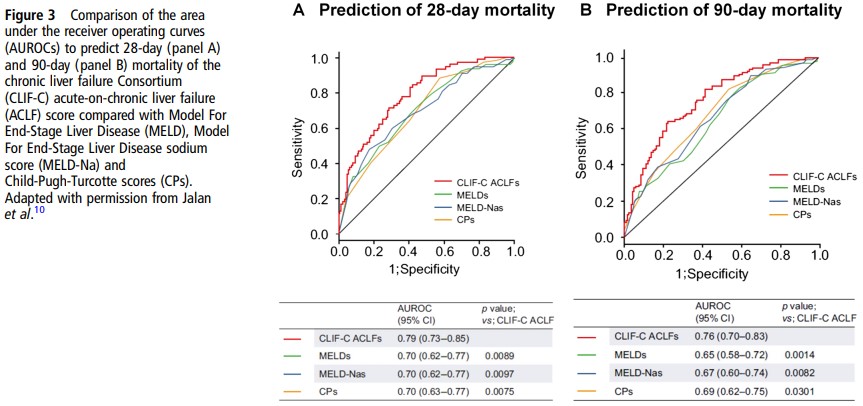
the intensive care unit (ICU) and also to have a rational basis to to decide futility.CLIF-C: a liver-specific score to predict outcomes in ACLFUntil recently, MELD score, MELD-Na and Child-Pugh Turcotte scores, the conventional scoring systems to assess prognosis in patients with cirrhosis, were the only available methods to evaluate prognosis in patients with ACLF.Besides being useful to determine the presence or absence of ACLF, CLIF SOFA and CLIF-C OF score were also found to be associated with prognosis.9 10 The performance of CLIF-C OFs in predicting shortterm mortality was similar to that of CLIF-SOFA score and slightly but significantly superior to MELD, MELD-Na and Child-Pugh-Turcotte scores.10