
In this post I link to and excerpt from:
- #202 LIVE! Lymphadenopathy: A PRACTICAL APPROACH TO LYMPHADENOPATHY WITH CARRIE THOMPSON MD, HEMATOLOGY-ONCOLOGY. MARCH 30, 2020 By MATTHEW WATTO, MD of The Curbsiders [Link is to the Episode List].
Here are excerpts:
Lymphadenopathy Pearls
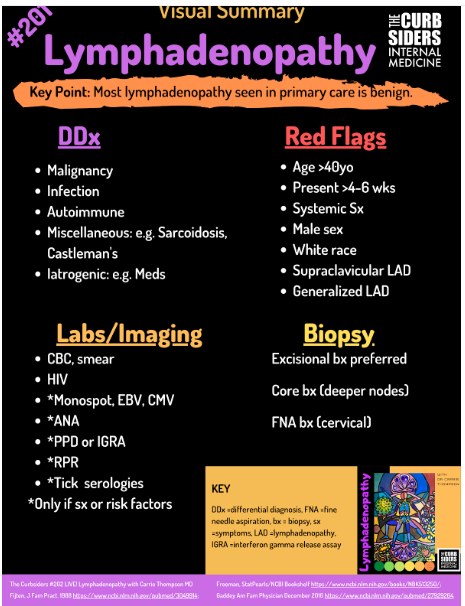
- Most lymphadenopathy (LAD) seen in primary care is not caused by malignancy.
- No physical exam signs can differentiate benign from malignant.
- Initial labs: CBC with differential, Peripheral smear, HIV.
- Additional tests to consider: ANA, EBV, CMV, Monospot, RPR, Hep B sAg, TB testing, Serology for tick borne illness if risk factors.
- Flow cytometry on peripheral blood is usually unhelpful in the workup for LAD since lymphomas are a disease of the lymph nodes and do not have abnormal circulating lymphocytes.
- Imaging: CT scan is usually the first choice for adults because it delineates the extent of LAD including deeper lymph node involvement. Ultrasound is preferred in pediatrics.
- Biopsy: Excisional lymph node biopsy preferred if lymphoma suspected. Biopsy the largest palpable lymph node. Core needle biopsy preferred for deeper, non-palpable nodes.
Differential Diagnosis (DDx) for Lymphadenopathy
Most lymphadenopathy (LAD) seen in primary care is not caused by malignancy, which makes up about 4% in those over 40 and 0.4% of those under 40 years old [Fitjen, 1988*]. NOTE*: This was a small retrospective study from the Netherlands. We wouldn’t put too much stock in percentages, but the general consensus is that the rate of malignant LAD in primary care is low.
MIAMI Mnemonic
Mnemonic suggested by Gaddey, 2016
- Malignancy
- Infection -probably the most common cause for LAD.
- Autoimmune e.g. SLE, RA
- Miscellaneous e.g. Castleman’s*, sarcoidosis**
- * Castleman Disease from emedicine.medscape.com
- ** Sarcoidosis from emedicine.medscape.com
- Iatrogenic e.g. allopurinol, anti-epileptic drugs, beta blockers
Taking a history for lymphadenopathy
Use the ALL AGES Mnemonic
Mnemonic suggested by Dr. Thompson
- Age
- Location
- Length of time present -most reactive nodes are gone in 2 weeks or so.
- Associated symptoms e.g. fever, wt loss
- Generalized or localized?
- Extranodal associations e.g. joint pain, rash
- Splenomegaly
Red Flags
As suggested by Gaddey, 2016
- Older age, usually >40 yo because about 4% of these patients will have malignancy [Fitjen, 1988]
- Present more than 4-6 weeks (or not to baseline by 8-12 weeks)
- Male sex
- White race
- Supraclavicular location, which drains the lungs, GI tract and GU system
- Systemic symptoms (e.g. wt loss, fevers)
- Generalized LAD (more than 2 regions) is more likely to be malignant than localized LAD, which is often infection.
Physical exam
Dr. Thompson recommends checking for lymphadenopathy as part of the routine exam (expert opinion). Check for cervical, supraclavicular, axillary and inguinal lymphadenopathy.
- Any palpable nodes are abnormal.
- No physical exam signs can differentiate benign from malignant.
- Shotty LAD refers to pea sized or smaller. Usually benign.
Lab studies in lymphadenopathy
Dr. Thompson recommends obtaining the following lab studies to evaluate lymphadenopathy:
- CBC with differential
- Peripheral smear
- HIV
The following additional tests can be considered if clinical suspicion is high (list based on both Gaddey, 2016 algorithm and our conversation with Dr. Thompson):
- +/-EBV, CMV, Monospot if viral symptoms
- +/- ANA, ONLY IF history is suggestive of an autoimmune condition
- +/- PPD or IGRA if TB risk factors
- +/- RPR
- +/- Hep B sAg
- +/- Serology for tick borne illness if risk factors
Imaging
Dr. Thompson notes that a CT scan is usually the first choice for adults because it delineates the extent of LAD including deeper lymph node involvement. Ultrasound can be helpful to avoid radiation in pediatric patients or to help plan for a needle biopsy in adults.
Biopsy for Lymphadenopathy
Fine needle aspiration (FNA) acquires a small piece of tissue to examine the cell type present i.e. malignant vs benign. Dr. Thompson might choose an FNA if a patient has cervical or supraclavicular adenopathy and lung cancer or head & neck cancer is suspected because an excisional biopsy in these cases might make future neck dissection more difficult (expert opinion).
A core needle biopsy is larger and gives some idea of the histopathology i.e. “what the cells look like in place next to each other”. This is most useful for non-palpable lymph nodes (expert opinion).
Excisional biopsy gives the lymph node’s entire architecture and is particularly important in diagnosing lymphoma. For example, in Hodgkin’s lymphoma the pathognomonic Reed Sternberg cells are the minority of cells and, thus might be missed by an FNA or core needle biopsy (expert opinion).
Which lymph node should you biopsy?
Generally, Dr. Thompson recommends a biopsy of the largest palpable lymph node (LN). If equal size LNs in the inguinal and axillary region, then go with the axillary LN since they’re less likely reactive. If no palpable LN and significant internal LAD (e.g. mesenteric or mediastinal) then a core needle biopsy of these sites is appropriate (expert opinion).
When should a patient with LAD be referred to Heme Onc?
Usually the referral is made after a biopsy has been obtained, but one might consider referral for fever of unknown origin or to help interpret the initial biopsy results.



