
In this post I link to and excerpt from Emergency Medicine Cases’ ECG Cases 12: RBBB and Occlusion MI. Written by Jesse McLaren; Peer Reviewed and edited by Anton Helman. August 2020.
All that follows is from Dr. McLaren’s awesome post.
In this ECG Cases blog we look at 7 patients with RBBB and potentially ischemic symptoms. Which had RBBB and occlusion MI?
Seven patients presented with potentially ischemic symptoms. Which had occlusion MI?
RBBB and Occlusion MI
When the right bundle branch is blocked, the septum depolarizes (left to right) followed by rapid depolarization of the left ventricle via the left bundle branch, and then the right ventricle depolarizes slowly. So QRS is prolonged >120ms (incomplete RBBB if <120ms), right-sided precordial leads have RsR’ in V1 (R from septal depolarization, S from LV depolarization, and R’ from delayed RV depolarization), and left-side precordial leads have RS wave (with rapid R from LV depolarization, and slurred S from slower RV depolarization). Axis should be normal in RBBB, and an abnormal axis could be the clue to a concomitant left anterior fascicular block (left axis, qR in I/aVL and rS in II/III/aVF) or left posterior fascicular block (right axis, rS in I/aVL, qR in III/aVF), or another reason for altered axis.
The right bundle runs down the interventricular septum and gets most of its blood supply from the LAD. So acute RBBB can develop if the septum is stretched by acute RV strain (from PE), or from acute coronary occlusion (especially of the LAD). RBBB in acute coronary occlusion can be pre-existing (more likely in older patients with comorbidities) or it can be acute, where it’s associated with larger infarcts, higher rates of heart failure and heart block, and higher mortality. While “new LBBB” is no longer considered a “STEMI equivalent”, there’s increasing recognition of the dangers of new RBBB in the context of acute coronary occlusion. Mortality from STEMI is higher in new RBBB compared to new LBBB, and higher still in bifascicular block—most commonly RBBB + LAFB, because of the left anterior fascicle is thinner and has more susceptible to ischemia than the left posterior fascicle [1]. While diffuse STD with reciprocal STE-aVR was once equated with left main occlusion, it’s now recognized to have a muchbroader differential diagnosis, but new RBBB+LAFB+STEMI has been associated with left main occlusion.[2]
As with other causes of abnormal depolarization, RBBB causes repolarization abnormalities that can mask or mimic ischemic changes (especially in right-sided precordial leads that have RSR’), but the concept of appropriate discordance can help. As a review summarized: “The major, terminal portion of the QRS complex and the initial portion of the ST segment/T wave are discordant, meaning that they are located on opposite sides of the isoelectric baseline. Thus, in the right to mid precordial leads, the largely positive QRS complex will be associated with ST-segment depression and an inverted T wave. A ‘violation’ of this concept will manifest as ST-segment elevation, which is concordant with the major, terminal portion of the QRS complex; the T-wave findings are often variable with either continued inversion or disappearance (lost within the greater ST segment itself). Anterior wall STEMI is therefore usually quite obvious if the clinician is comfortable with the appropriate appearance of the ST segment in RBBB.”[3] But sometimes ECG changes can be subtle or non-existent. As with the guideline for PCI in patients with refractory ischemia, the 2017 European Society of Cardiology advises, “Patients with MI and right bundle branch block (RBBB) have a poor prognosis. It may be difficult to detect transmural ischaemia in patients with chest pain and RBBB. Therefore, a primary PCI strategy (emergent coronary angiography and PCI if indicated) should be considered when persistent ischaemic symptoms occur in the presence of RBBB.”[4]
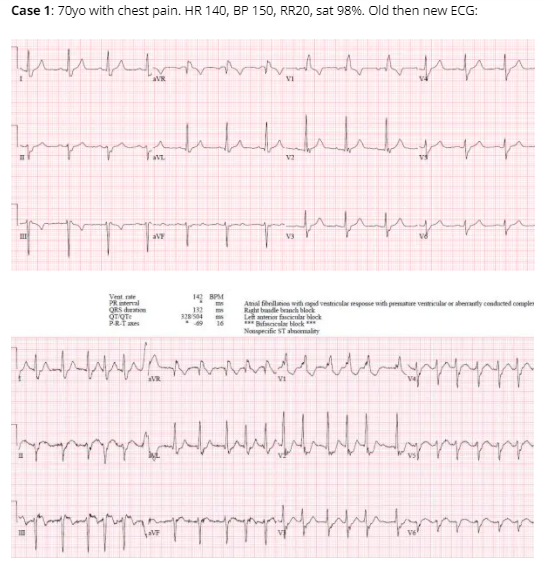
Case 1: unnecessary cath lab activation
Old RBBB+LAFB, new rapid atrial fibrillation and rate-related ST changes. Cath lab activated based on mild inferior ST elevation, but ST changes resolved with rate control. Mild troponin elevation from non-occlusive MI.



