
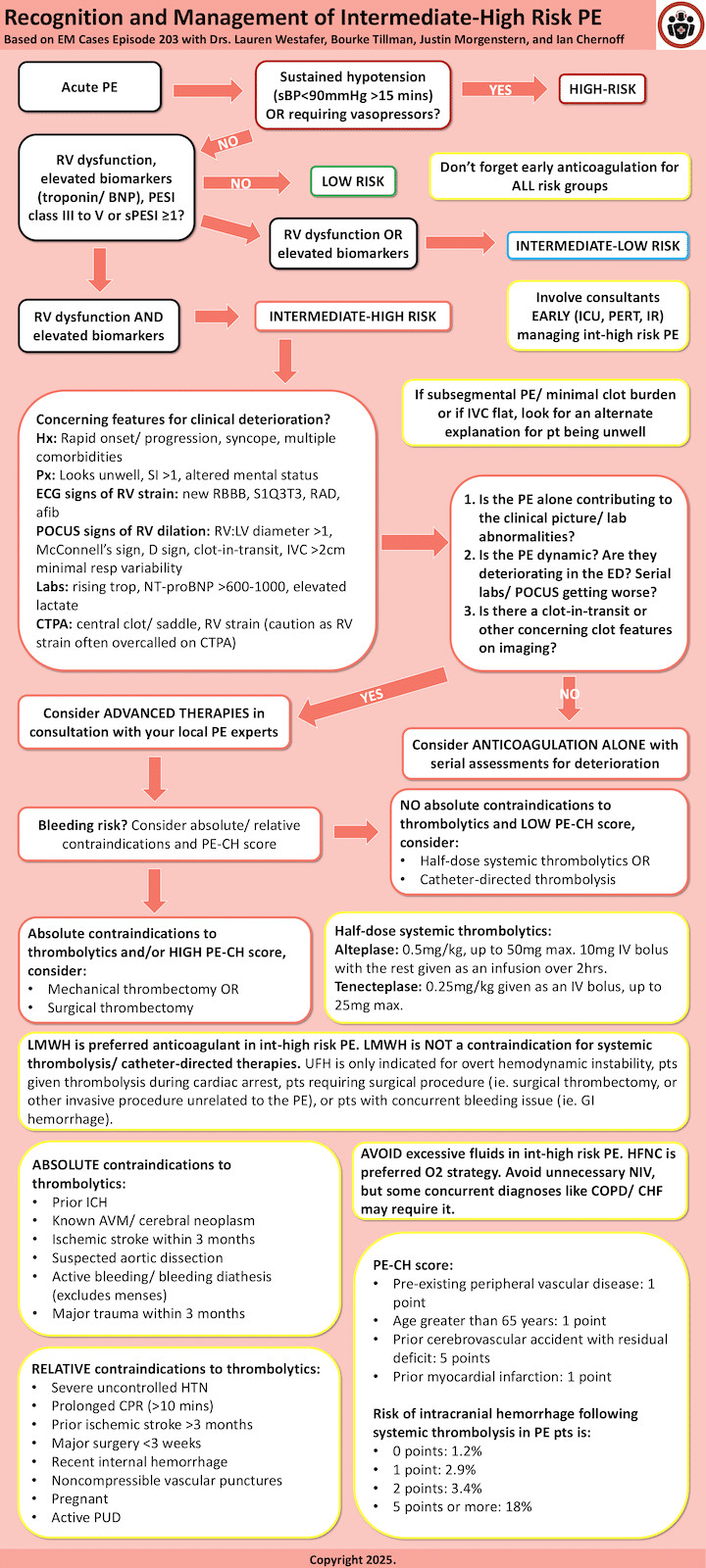
In addition to today’s resource, I link to and embed the flow chart from Emergency Medicine Cases Ep 203 Intermediate Risk Pulmonary Embolism Risk Stratification, Management and Algorithm:*
*Helman, A. Morgenstern, J. Tillmann, B. Westafer, L. Intermediate Risk Pulmonary Embolism Risk Stratification, Management and Algorithm. Emergency Medicine Cases. Month, 2024. https://emergencymedicinecases.com/intermediate-risk-pulmonary-embolism-risk-stratification-management. Accessed May 7, 2025
Today, I review, link to, and excerpt from First10EM‘s Management of intermediate and high risk pulmonary embolism (aka submassive/massive PE).*
*Morgenstern, J. Management of intermediate and high risk pulmonary embolism (aka submassive/massive PE), First10EM, April 1, 2025. Available at:
https://doi.org/10.51684/FIRS.140873
Note to myself and my readers: Dr. Morganstern’s post is outstanding and should be read in its entirety. I just excerpted some of his points.
All that follows is from the above resource.
Pulmonary embolism is probably discussed far more than is truly necessary. It receives more attention than almost any other pathology. We endlessly debate the best algorithms for diagnosis. We add new decision tools almost yearly. However, if there is one aspect of pulmonary embolism that might be under-discussed it is the management of massive and submissive PEs. After being asked to participate in an Emergency Medicine Cases podcast on the subject*, I spent a lot of time on PubMed trying to fill gaps in my knowledge. These are the notes that I made for that podcast.
*Helman, A. Morgenstern, J. Tillmann, B. Westafer, L. Intermediate Risk Pulmonary Embolism Risk Stratification, Management and Algorithm. Emergency Medicine Cases. Month, 2024. https://emergencymedicinecases.com/intermediate-risk-pulmonary-embolism-risk-stratification-management. Accessed May 4, 2025
When should we be using thrombolysis?
There is general agreement that thrombolysis should be used in patients with massive PE, which is defined as patients having hypotension. As a whole the data is not strong, and there is definitely remaining uncertainty, but the absolute benefit in massive PE looks large enough to drive clinical practice. For example, in one systematic review and meta-analysis that includes 748 patient from 11 trials, although there was no overall statistical benefit from thrombolytics, the subgroup of massive (or hemodynamically unstable) PE demonstrated a 10% absolute reduction in mortality (9.4% versus 19.0%; OR 0.45, 95% CI 0.22 to 0.92; number needed to treat=10). (Wan 2004)
Reading through some of these early trials, “life threatening” or “hemodynamically unstable” PE was often left undefined. Clinically, the working definition seems to be focused on hypotension, although even the exact definition of hypotension is somewhat unclear (especially in the initial chaos of an emergency resuscitation). Consensus definitions of massive PE, and therefore clear indications for thrombolysis, usually include: (Jaff 2011; Konstantinides 2014; Kearon 2016)
- Systolic BP < 90 mm for 15 minutes.
- Fall in systolic BP by >40 mm for 15 minutes.
- Requirement for vasopressors.
Thrombolysis as first line therapy for massive PE is supported by several international guidelines, including those from the ACCP, AHA, ESC, and ACEP. (Jaff 2011; Kearon 2016; Konstantinides 2020)
“Submassive PE” encompasses a much larger and much more heterogeneous group of patients, which probably explains why there is still so much confusion and debate about the best approach to these patients. Hopefully future research will do a better job risk stratifying within this group, because they are not all created equal. For now, management will require a lot of clinical judgment, based on a number of factors.
A quick aside: why are we giving thrombolytics?
As emergency and critical care physicians, we are often focused on the immediate question of whether a patient is going to live or die. Unfortunately, even when our patients survive the initial insult, there are often long term consequences of their pathology. For DVT, a significant minority of patients have chronic symptoms from post-thrombotic syndrome. Similarly, after pulmonary embolism, many patients have significant long term pulmonary hypertension and persistent dyspnea reducing their quality of life.
There was some thought that thrombolysis might improve the long term outcomes after PE, but long term follow-up of the PEITHO trial (discussed more below) demonstrated no change in mortality, functional limitations, or pulmonary hypertension at 3 year follow up. Therefore, for the time being, if we are considering thrombolysis in the setting of PE, we are doing so to prevent short term clinical deterioration or death. (Konstantinides 2017)
Back to the main question: which submassive PEs should be treated with thrombolysis? (The evidence)
As of 2024, there is no definitive answer to which submissive PE patients (if any) will benefit from thrombolysis. There are conflicting meta-analyses and conflicting points of view. For the most part, we just don’t have enough studies focused on differentiating this very heterogeneous group.
So who do I actually treat?
The intermediate or submissive group of patients is incredibly variable, and specific evidence to guide treatment is still mostly lacking. This group is defined differently in different guidelines, with the key features usually being either evidence or right ventricular dysfunction and/or changes in biomarkers such as troponin or BNP. Most publications lump all the patients together, but some try to stratify them further. For example, the ESC guidelines call patients “intermediate low risk” if they have either right ventricular dysfunction or positive biomarkers, and “intermediate high risk” if they have both. (Machanahalli Balakrishna 2022)
Within this intermediate group, there are almost certainly high risk patients, closer to the “massive” group, who warrant thrombolysis, while there are other patients who are much lower risk and would be harmed by thrombolysis. Unfortunately, within the intermediate risk or “submassive” group, there is no single variable that will make this decision for you. You are going to have to make a judgment call that incorporates many clinical variables.
After reviewing all this evidence, I don’t think I can improve much on the PulmCrit/IBCC risk stratification, so I will just copy and paste his schema here:
His scheme (and this article) isn’t really focused on the low risk patients, and there are numerous other factors that you will consider if you are thinking about sending a patient home (bleeding risk, current anticoagulation, renal function, liver disease, social issues, etc), but that is a topic for another time.
The key to this schema is that the management of submassive PE is nuanced. In the high risk submassive patients, there will be a consideration of advanced therapies, but based on the uncertainty in the current literature, this is usually not a decision I will make on my own in the emergency department. I like Farkas’ algorithm because it reminds us of the importance of re-evaluation in the lower-risk submassive patients, and the value of ICU admission and consultation in the higher risk patients.
One key point that doesn’t make it into this graphic: although we rarely use unfractionated heparin anymore, these submissive PE patients should all start on unfractionated heparin, because if they deteriorate or require thrombolytic therapy, that is much safer when unfractionated heparin has been used. (Although listen to the EMCases podcast on the topic, where Lauren Westafer presents very strong opinions to the contrary.)
Contraindications
Of course, the standard contraindications of thrombolysis still apply. That being said, most contraindications are relative rather than absolute. If a patient is peri-arrest, the benefits of thrombolysis are probably going to outweigh the harms. On the other hand, with no clear evidence of benefit in the submassive group of patients, any contra-indication needs to be taken seriously. The exact list of conta-indications and whether they are “absolute” or “relative” varies between guidelines.
I find the terminology of “absolute” and “relative” to be clinically useless, as there is really no such thing as an absolute contraindication, and relative is only helpful if accompanied by some estimate of risk of hemorrhage. Ideally, each of these risk factors would be listed with their individual risk of harm. Barring that, I like the breakdown that Scott Weingart uses,* instead breaking patients into high, moderate, and low risk for bleeding, and proceeding accordingly.
*The pathway below is bigger and easier t0 read in the above link.
What about catheter directed thrombolysis?
My instinct is that, given that the entire circulating blood volume goes through the lungs (as compared to the small fraction that goes through the cerebral or coronary arteries), there should be no advantage to giving thrombolytics through a specialized catheter as compared to a peripheral IV. Clot retrieval makes more sense, but thus far has shown no benefit.
Bottom line: I don’t think there is any reason to use catheter directed thrombolysis or “ultrasound facilitated thrombolysis” at this time. There is no good evidence, and they don’t make physiologic sense. Using interventional radiology techniques to mechanically retrieve the clot might make more sense, and are discussed below, but also have absolutely no evidence supporting them at this time.
There are a number of ongoing studies in this area, but unfortunately almost all of them seem to be poorly designed.
What is the thrombolytic dose for cardiac arrest?
The recommendations around thrombolytics during cardiac arrest tend to focus on the PEAPETT study, in which 23 patients with confirmed pulmonary embolism and PEA arrest were treated with a 50 mg IV push of tPa, and return of spontaneous circulation was achieved in 22 of the 23 patients. (Sharifi 2016) 21 of the 23 patients survived to hospital discharge and 20 (87%) were still alive at 3 month follow-up, which is an unheard of number for PEA arrest. Obviously, without a control group, the conclusions are limited.
Therefore, in an arrest, my current approach is to give tPa as a 50 mg IV bolus, and I am willing to repeat that bolus once if unsuccessful.
As mentioned above, the outcomes for PE patients treated with thrombolytics are much better than for almost any other cause of PEA arrest. I think that is the logic that leads to the ESC guideline to recommend “once a thrombolytic drug is administered, cardiopulmonary resuscitation should be continued for at least 60-90 min before terminating resuscitation attempts.” (Konstantinides 2020) That time frame seems unrealistic to me, but you certainly need to run these codes longer than you are used to.
How do you resuscitate a patient with a massive / submassive PE?
A sick patient with pulmonary embolism is in right ventricular failure, which, as we have covered before, is an incredibly high risk scenario. We need to be incredibly careful about anything that could either increase pulmonary artery pressures or impair RV perfusion, which means meticulously avoiding hypoxia, hypercapnia, positive pressure ventilation, and hypotension.
A general lesson that I took away from this literature is that we should always be prepared for these patients to deteriorate or arrest, but when they do, we should be more aggressive than usual (or at least more willing to run a prolonged code) because outcomes seem to be good. In the PEAPETT study that looked at tPa during PEA arrest, 87% of the patients were still alive at 3 months. (Sharifi 2016) In the MAPPET study, 35% of the patients who received CPR survived to hospital discharge. (Kasper 1997) Those are much higher numbers than we are used to, especially in PEA arrests, so although our goal should be resuscitating in a manner that avoids arrest, we should also be optimistic and aggressive if an arrest does occur.
Airway
An endotracheal tube is not a solution to massive pulmonary embolism. Plastic between the cords will not solve the issue, even if there is hypoxia. On the other hand, everything we do to intubated patients, from the medications we give them, to the peri-intubation risk of hypoxia and hypercapnia, to the transition to positive pressure ventilation, has the potential to kill these patients. In general, our goal is to avoid intubation. Consider all alternatives, such as high flow nasal oxygen, before intubation.
Massive pulmonary embolism causes acute pulmonary hypertension and acute right heart failure. I have an entire post dedicated to the management of pulmonary hypertension and right heart failure, but the conclusion there is the same: if at all possible, do not intubate.
If an intubation is absolutely required, it should be an awake intubation (or, realistically for most departments, a ketamine facilitated breathing intubation).
Fluids
Avoid fluid resuscitation
No one is going to fault you for trying a little fluid resuscitation in a hypotensive patient, but when dealing with a massive PE, they are more likely to harm than help. (Konstantinides 2020) The RV is already overloaded. Further stretch will make things worse by increasing tricuspid regurgitation, pushing the septum in the left ventricle, decreasing LV output, and increasing tension on the RV wall, which impairs perfusion and increases ischemia.
If the patient is fluid responsive, or if there is a small IVC on ultrasound, you probably aren’t dealing with a hemodynamically consequential PE. If you know it is a hemodynamically consequential PE, avoid IV fluids.
Pressors
Aside from pretty strong data that dopamine is a bad choice in all clinical settings, we really don’t have strong data comparing (or even really supporting) vasopressors. I don’t think you would be wrong for starting with your usual choice of norepinephrine, but some experts suggest epinephrine as the vasopressor of choice in massive PE for theoretical reasons (the beta activity might cause pulmonary vasodilation, these patients almost certainly need inotropy in addition to pure vasoconstriction, and bradycardia is common in the pre-arrest stage). Vasopressin might also have beneficial effects in the setting of pulmonary hypertension, but is harder to titrate, and so is probably relegated to a second line agent. (Condliffe 2017; Joshi 2022)
Plan ahead
A really important part of caring for critically ill patients is being cognizant of next steps, especially if the patient deteriorates. We are usually really good at this, involving specialists or arranging transfers early, even if the patient doesn’t necessarily need their care right now. One thing to keep in mind with the sick PE patient is the chance of thrombolysis in the near future, even if you decide not to prescribe it immediately. Consider the impact of thrombolysis on the procedures you are performing. There is almost never a reason to perform an ABG, but avoiding arterial sticks makes even more sense if you are going to use a thrombolytic. We know peripheral vasopressors are a fine option, so there is no need for an inexperienced proceduralist to perform an immediate central line. If you are placing a central line, put it in a compressible location.
Surgical thrombectomy
Bottom line: There is very little evidence, the outcomes don’t seem great, and it is rarely available. However, in a very sick patient with contraindications to thrombolysis, it is worth having a discussion with a vascular surgeon.
What anticoagulant is best for submissive PE?
Bottom line: There really is not good evidence for anticoagulation in PE, and it probably does require large high quality RCTs, especially starting in the lowest risk patients we diagnose. That being said, it is clearly the current standard, and we are all proceeding with anticoagulation until we see better data.
OK, enough of the EBM BS. How do I actually anticoagulate?
The key when deciding about anticoagulation is to remember that you are not treating the current clot burden, but trying to prevent more clot from forming.
Low molecular weight heparin (LMWH) is no more effective than unfractionated heparin, but does consistently demonstrate less bleeding. For the average low risk patient, LMWH is the way to go, if you are starting with heparin. However, this article is focused on high risk patients, and the major advantage of unfractionated heparin is that it can be stopped, titrated, and reversed. If there is any chance that a patient is going to need thrombolysis or a procedure for their PE in the next 24 hours, I would choose unfractionated heparin over LMWH. Most guidelines don’t make this point, but Thrombosis Canada specifically says if “thrombolysis is being considered … intravenous (IV) UFH is preferred in the short-term due to its short half-life in the context of the bleeding risk associated with thrombolysis.” (Thrombosis Canada 2023)
Other FOAMed
PulmCrit IBCC: Submassive & Massive PE
PulmCrit- Inhaled NO for submassive PE: iNOPE or iYEP?
Eight pearls for the crashing patient with massive PE
Pulmonary hypertension and right ventricular failure – The first 10 minutes
REBELEM: The Critical Pulmonary Embolism Patient
EMCrit RACC Pulmonary Embolism Pathway
PEERLESS: Interventional therapies for pulmonary embolism
References
Aykan A, Gökdeniz T, Gül, et al. Reduced-Dose Systemic Fibrinolysis in Massive Pulmonary Embolism: A Pilot Study Clin Exp Emerg Med. 2023; 10(3):280-286.
Bajaj A, Saleeb M, Rathor P, Sehgal V, Kabak B, Hosur S. Prognostic value of troponins in acute nonmassive pulmonary embolism: A meta-analysis. Heart Lung. 2015 Jul-Aug;44(4):327-34. doi: 10.1016/j.hrtlng.2015.03.007. Epub 2015 May 11. PMID: 25976228
Barco S, Ende-Verhaar YM, Becattini C, Jimenez D, Lankeit M, Huisman MV, Konstantinides SV, Klok FA. Differential impact of syncope on the prognosis of patients with acute pulmonary embolism: a systematic review and meta-analysis. Eur Heart J. 2018 Dec 14;39(47):4186-4195. doi: 10.1093/eurheartj/ehy631. PMID: 30339253
BARRITT DW, JORDAN SC. Anticoagulant drugs in the treatment of pulmonary embolism. A controlled trial. Lancet. 1960 Jun 18;1(7138):1309-12. doi: 10.1016/s0140-6736(60)92299-6. PMID: 13797091
Becattini C, Agnelli G, Salvi A, Grifoni S, Pancaldi LG, Enea I, Balsemin F, Campanini M, Ghirarduzzi A, Casazza F; TIPES Study Group. Bolus tenecteplase for right ventricle dysfunction in hemodynamically stable patients with pulmonary embolism. Thromb Res. 2010 Mar;125(3):e82-6. doi: 10.1016/j.thromres.2009.09.017. Epub 2009 Oct 14. PMID: 19833379
Boone JD, Sherwani SS, Herborn JC, Patel KM, De Wolf AM. The successful use of low-dose recombinant tissue plasminogen activator for treatment of intracardiac/pulmonary thrombosis during liver transplantation. Anesth Analg. 2011 Feb;112(2):319-21. doi: 10.1213/ANE.0b013e31820472d4. Epub 2010 Dec 2. PMID: 21127275
Carroll BJ, Beyer SE, Mehegan T, Dicks A, Pribish A, Locke A, Godishala A, Soriano K, Kanduri J, Sack K, Raber I, Wiest C, Balachandran I, Marcus M, Chu L, Hayes MM, Weinstein JL, Bauer KA, Secemsky EA, Pinto DS. Changes in Care for Acute Pulmonary Embolism Through A Multidisciplinary Pulmonary Embolism Response Team. Am J Med. 2020 Nov;133(11):1313-1321.e6. doi: 10.1016/j.amjmed.2020.03.058. Epub 2020 May 19. PMID: 32416175
Chatterjee S, Chakraborty A, Weinberg I, Kadakia M, Wilensky RL, Sardar P, Kumbhani DJ, Mukherjee D, Jaff MR, Giri J. Thrombolysis for pulmonary embolism and risk of all-cause mortality, major bleeding, and intracranial hemorrhage: a meta-analysis. JAMA. 2014 Jun 18;311(23):2414-21. doi: 10.1001/jama.2014.5990. PMID: 24938564
Chaudhury P, Gadre SK, Schneider E, Renapurkar RD, Gomes M, Haddadin I, Heresi GA, Tong MZ, Bartholomew JR. Impact of Multidisciplinary Pulmonary Embolism Response Team Availability on Management and Outcomes. Am J Cardiol. 2019 Nov 1;124(9):1465-1469. doi: 10.1016/j.amjcard.2019.07.043. Epub 2019 Aug 7. PMID: 31495443
Condliffe R, Kiely D. Critical care management of pulmonary hypertension BJA Education. 2017; 17(7):228-234.
Cundiff DK, Manyemba J, Pezzullo JC. Anticoagulants versus non-steroidal anti-inflammatories or placebo for treatment of venous thromboembolism. Cochrane Database Syst Rev. 2006 Jan 25;2006(1):CD003746. doi: 10.1002/14651858.CD003746.pub2. PMID: 16437461
Fernandes P, Allen P, Valdis M, Guo L. Successful use of extracorporeal membrane oxygenation for pulmonary embolism, prolonged cardiac arrest, post-partum: a cannulation dilemma. Perfusion. 2015 Mar;30(2):106-10. doi: 10.1177/0267659114555818. Epub 2014 Oct 10. PMID: 25304130
Jaber WA, Gonsalves CF, Stortecky S, Horr S, Pappas O, Gandhi RT, Pereira K, Giri J, Khandhar SJ, Ammar KA, Lasorda DM, Stegman B, Busch L, Dexter DJ 2nd, Azene EM, Daga N, Elmasri F, Kunavarapu CR, Rea ME, Rossi JS, Campbell J, Lindquist J, Raskin A, Smith JC, Tamlyn TM, Hernandez GA, Rali P, Schmidt TR, Bruckel JT, Camacho JC, Li J, Selim S, Toma C, Basra SS, Bergmark BA, Khalsa B, Zlotnick DM, Castle J, O’Connor DJ, Gibson CM; PEERLESS Committees and Investigators*. Large-Bore Mechanical Thrombectomy Versus Catheter-Directed Thrombolysis in the Management of Intermediate-Risk Pulmonary Embolism: Primary Results of the PEERLESS Randomized Controlled Trial. Circulation. 2025 Feb 4;151(5):260-273. doi: 10.1161/CIRCULATIONAHA.124.072364. Epub 2024 Oct 29. PMID: 39470698
Jaff MR, McMurtry MS, Archer SL, Cushman M, Goldenberg N, Goldhaber SZ, Jenkins JS, Kline JA, Michaels AD, Thistlethwaite P, Vedantham S, White RJ, Zierler BK; American Heart Association Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation; American Heart Association Council on Peripheral Vascular Disease; American Heart Association Council on Arteriosclerosis, Thrombosis and Vascular Biology. Management of massive and submassive pulmonary embolism, iliofemoral deep vein thrombosis, and chronic thromboembolic pulmonary hypertension: a scientific statement from the American Heart Association. Circulation. 2011 Apr 26;123(16):1788-830. doi: 10.1161/CIR.0b013e318214914f. PMID: 21422387
Joshi S, Quinones Cardona V, Menkiti OR. Use of vasopressin in persistent pulmonary hypertension of the newborn: A case series SAGE Open Medical Case Reports. 2022; 10:2050313X2211022-.
Kasper W, Konstantinides S, Geibel A, Olschewski M, Heinrich F, Grosser KD, Rauber K, Iversen S, Redecker M, Kienast J. Management strategies and determinants of outcome in acute major pulmonary embolism: results of a multicenter registry. J Am Coll Cardiol. 1997 Nov 1;30(5):1165-71. doi: 10.1016/s0735-1097(97)00319-7. PMID: 9350909
Kawahito K, Murata S, Adachi H, Ino T, Fuse K. Resuscitation and circulatory support using extracorporeal membrane oxygenation for fulminant pulmonary embolism. Artif Organs. 2000 Jun;24(6):427-30. doi: 10.1046/j.1525-1594.2000.06590.x. PMID: 10886059
Kearon C, Akl EA, Ornelas J, Blaivas A, Jimenez D, Bounameaux H, Huisman M, King CS, Morris TA, Sood N, Stevens SM, Vintch JRE, Wells P, Woller SC, Moores L. Antithrombotic Therapy for VTE Disease: CHEST Guideline and Expert Panel Report. Chest. 2016 Feb;149(2):315-352. doi: 10.1016/j.chest.2015.11.026. Epub 2016 Jan 7. Erratum in: Chest. 2016 Oct;150(4):988. doi: 10.1016/j.chest.2016.08.1442. PMID: 26867832
Keeling WB, Sundt T, Leacche M, Okita Y, Binongo J, Lasajanak Y, Aklog L, Lattouf OM; SPEAR Working Group. Outcomes After Surgical Pulmonary Embolectomy for Acute Pulmonary Embolus: A Multi-Institutional Study. Ann Thorac Surg. 2016 Nov;102(5):1498-1502. doi: 10.1016/j.athoracsur.2016.05.004. Epub 2016 Jun 30. PMID: 27373187
Kiser TH, Burnham EL, Clark B, Ho PM, Allen RR, Moss M, Vandivier RW. Half-Dose Versus Full-Dose Alteplase for Treatment of Pulmonary Embolism. Crit Care Med. 2018 Oct;46(10):1617-1625. doi: 10.1097/CCM.0000000000003288. PMID: 29979222
Kline JA, Hernandez J, Garrett JS, Jones AE. Pilot study of a protocol to administer inhaled nitric oxide to treat severe acute submassive pulmonary embolism. Emerg Med J. 2014 Jun;31(6):459-62. doi: 10.1136/emermed-2013-202426. Epub 2013 Apr 13. PMID: 23585574
Kline JA, Nordenholz KE, Courtney DM, Kabrhel C, Jones AE, Rondina MT, Diercks DB, Klinger JR, Hernandez J. Treatment of submassive pulmonary embolism with tenecteplase or placebo: cardiopulmonary outcomes at 3 months: multicenter double-blind, placebo-controlled randomized trial. J Thromb Haemost. 2014 Apr;12(4):459-68. doi: 10.1111/jth.12521. PMID: 24484241
Kline JA, Puskarich MA, Jones AE, Mastouri RA, Hall CL, Perkins A, Gundert EE, Lahm T. Inhaled nitric oxide to treat intermediate risk pulmonary embolism: A multicenter randomized controlled trial. Nitric Oxide. 2019 Mar 1;84:60-68. doi: 10.1016/j.niox.2019.01.006. Epub 2019 Jan 8. PMID: 30633959
Konstantinides S, Geibel A, Heusel G, Heinrich F, Kasper W; Management Strategies and Prognosis of Pulmonary Embolism-3 Trial Investigators. Heparin plus alteplase compared with heparin alone in patients with submassive pulmonary embolism. N Engl J Med. 2002 Oct 10;347(15):1143-50. doi: 10.1056/NEJMoa021274. PMID: 12374874
Konstantinides SV, Torbicki A, Agnelli G, Danchin N, Fitzmaurice D, Galiè N, Gibbs JS, Huisman MV, Humbert M, Kucher N, Lang I, Lankeit M, Lekakis J, Maack C, Mayer E, Meneveau N, Perrier A, Pruszczyk P, Rasmussen LH, Schindler TH, Svitil P, Vonk Noordegraaf A, Zamorano JL, Zompatori M; Task Force for the Diagnosis and Management of Acute Pulmonary Embolism of the European Society of Cardiology (ESC). 2014 ESC guidelines on the diagnosis and management of acute pulmonary embolism. Eur Heart J. 2014 Nov 14;35(43):3033-69, 3069a-3069k. doi: 10.1093/eurheartj/ehu283. PMID: 25173341
Konstantinides SV, Vicaut E, Danays T, Becattini C, Bertoletti L, Beyer-Westendorf J, Bouvaist H, Couturaud F, Dellas C, Duerschmied D, Empen K, Ferrari E, Galiè N, Jiménez D, Kostrubiec M, Kozak M, Kupatt C, Lang IM, Lankeit M, Meneveau N, Palazzini M, Pruszczyk P, Rugolotto M, Salvi A, Sanchez O, Schellong S, Sobkowicz B, Meyer G. Impact of Thrombolytic Therapy on the Long-Term Outcome of Intermediate-Risk Pulmonary Embolism. J Am Coll Cardiol. 2017 Mar 28;69(12):1536-1544. doi: 10.1016/j.jacc.2016.12.039. PMID: 28335835
Konstantinides SV, Meyer G, Becattini C, Bueno H, Geersing GJ, Harjola VP, Huisman MV, Humbert M, Jennings CS, Jiménez D, Kucher N, Lang IM, Lankeit M, Lorusso R, Mazzolai L, Meneveau N, Ní Áinle F, Prandoni P, Pruszczyk P, Righini M, Torbicki A, Van Belle E, Zamorano JL; ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur Heart J. 2020 Jan 21;41(4):543-603. doi: 10.1093/eurheartj/ehz405. PMID: 31504429
Kucher N, Boekstegers P, Müller OJ, Kupatt C, Beyer-Westendorf J, Heitzer T, Tebbe U, Horstkotte J, Müller R, Blessing E, Greif M, Lange P, Hoffmann RT, Werth S, Barmeyer A, Härtel D, Grünwald H, Empen K, Baumgartner I. Randomized, controlled trial of ultrasound-assisted catheter-directed thrombolysis for acute intermediate-risk pulmonary embolism. Circulation. 2014 Jan 28;129(4):479-86. doi: 10.1161/CIRCULATIONAHA.113.005544. Epub 2013 Nov 13. PMID: 24226805
Kuo WT, Banerjee A, Kim PS, DeMarco FJ Jr, Levy JR, Facchini FR, Unver K, Bertini MJ, Sista AK, Hall MJ, Rosenberg JK, De Gregorio MA. Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT): Initial Results From a Prospective Multicenter Registry. Chest. 2015 Sep;148(3):667-673. doi: 10.1378/chest.15-0119. PMID: 25856269
Lee T, Itagaki S, Chiang YP, Egorova NN, Adams DH, Chikwe J. Survival and recurrence after acute pulmonary embolism treated with pulmonary embolectomy or thrombolysis in New York State, 1999 to 2013. J Thorac Cardiovasc Surg. 2018 Mar;155(3):1084-1090.e12. doi: 10.1016/j.jtcvs.2017.07.074. Epub 2017 Aug 31. PMID: 28942971
Machanahalli Balakrishna A, Reddi V, Belford PM, Alvarez M, Jaber WA, Zhao DX, Vallabhajosyula S. Intermediate-Risk Pulmonary Embolism: A Review of Contemporary Diagnosis, Risk Stratification and Management. Medicina (Kaunas). 2022 Aug 30;58(9):1186. doi: 10.3390/medicina58091186. PMID: 36143863
Malekan R, Saunders PC, Yu CJ , et al. Peripheral extracorporeal membrane oxygenation: comprehensive therapy for high-risk massive pulmonary embolism. Ann Thorac Surg 2012; 94 (1) 104-108
Marti C, John G, Konstantinides S, Combescure C, Sanchez O, Lankeit M, Meyer G, Perrier A. Systemic thrombolytic therapy for acute pulmonary embolism: a systematic review and meta-analysis. Eur Heart J. 2015 Mar 7;36(10):605-14. doi: 10.1093/eurheartj/ehu218. Epub 2014 Jun 10. PMID: 24917641
Meyer G, Vicaut E, Danays T, Agnelli G, Becattini C, Beyer-Westendorf J, Bluhmki E, Bouvaist H, Brenner B, Couturaud F, Dellas C, Empen K, Franca A, Galiè N, Geibel A, Goldhaber SZ, Jimenez D, Kozak M, Kupatt C, Kucher N, Lang IM, Lankeit M, Meneveau N, Pacouret G, Palazzini M, Petris A, Pruszczyk P, Rugolotto M, Salvi A, Schellong S, Sebbane M, Sobkowicz B, Stefanovic BS, Thiele H, Torbicki A, Verschuren F, Konstantinides SV; PEITHO Investigators. Fibrinolysis for patients with intermediate-risk pulmonary embolism. N Engl J Med. 2014 Apr 10;370(15):1402-11. doi: 10.1056/NEJMoa1302097. PMID: 24716681
Nielsen HK, Husted SE, Krusell LR, Fasting H, Charles P, Hansen HH, Nielsen BO, Petersen JB, Bechgaard P. Anticoagulant therapy in deep venous thrombosis. A randomized controlled study. Thromb Res. 1994 Feb 15;73(3-4):215-26. doi: 10.1016/0049-3848(94)90100-7. PMID: 8191414
Ott P, Eldrup E, Oxholm P. Vaerdien af antikoagulansbehandling ved dyb venøs trombose i underekstremiteten hos den aeldre, mobiliserede patient. En dobbeltblind, placebokontrolleret undersøgelse med åben terapeutisk styring [Value of anticoagulant therapy in deep venous thrombosis in the lower limb in elderly, mobilized patients. A double-blind placebo controlled study with open therapeutic guidance]. Ugeskr Laeger. 1988 Jan 25;150(4):218-21. Danish. PMID: 3287734
Ozsu S, Erbay M, Durmuş ZG, Ozlu T. Classification of high-risk with cardiac troponin and shock index in normotensive patients with pulmonary embolism. J Thromb Thrombolysis. 2017 Feb;43(2):179-183. doi: 10.1007/s11239-016-1443-3. PMID: 27800569
Pastré J, Sanchis-Borja M, Benlounes M. Risk stratification and treatment of pulmonary embolism with intermediate-risk of mortality. Curr Opin Pulm Med. 2022 Sep 1;28(5):375-383. doi: 10.1097/MCP.0000000000000905. Epub 2022 Jul 18. PMID: 35855562
Piazza G, Hohlfelder B, Jaff MR, Ouriel K, Engelhardt TC, Sterling KM, Jones NJ, Gurley JC, Bhatheja R, Kennedy RJ, Goswami N, Natarajan K, Rundback J, Sadiq IR, Liu SK, Bhalla N, Raja ML, Weinstock BS, Cynamon J, Elmasri FF, Garcia MJ, Kumar M, Ayerdi J, Soukas P, Kuo W, Liu PY, Goldhaber SZ; SEATTLE II Investigators. A Prospective, Single-Arm, Multicenter Trial of Ultrasound-Facilitated, Catheter-Directed, Low-Dose Fibrinolysis for Acute Massive and Submassive Pulmonary Embolism: The SEATTLE II Study. JACC Cardiovasc Interv. 2015 Aug 24;8(10):1382-1392. doi: 10.1016/j.jcin.2015.04.020. PMID: 26315743
Qaddoura A, Digby GC, Kabali C, Kukla P, Zhan ZQ, Baranchuk AM. The value of electrocardiography in prognosticating clinical deterioration and mortality in acute pulmonary embolism: A systematic review and meta-analysis. Clin Cardiol. 2017 Oct;40(10):814-824. doi: 10.1002/clc.22742. Epub 2017 Jun 19. PMID: 28628222
Rivera-Lebron B, McDaniel M, Ahrar K, Alrifai A, Dudzinski DM, Fanola C, Blais D, Janicke D, Melamed R, Mohrien K, Rozycki E, Ross CB, Klein AJ, Rali P, Teman NR, Yarboro L, Ichinose E, Sharma AM, Bartos JA, Elder M, Keeling B, Palevsky H, Naydenov S, Sen P, Amoroso N, Rodriguez-Lopez JM, Davis GA, Rosovsky R, Rosenfield K, Kabrhel C, Horowitz J, Giri JS, Tapson V, Channick R; PERT Consortium. Diagnosis, Treatment and Follow Up of Acute Pulmonary Embolism: Consensus Practice from the PERT Consortium. Clin Appl Thromb Hemost. 2019 Jan-Dec;25:1076029619853037. doi: 10.1177/1076029619853037. PMID: 31185730
Sharifi M, Bay C, Skrocki L, Rahimi F, Mehdipour M; “MOPETT” Investigators. Moderate pulmonary embolism treated with thrombolysis (from the “MOPETT” Trial). Am J Cardiol. 2013 Jan 15;111(2):273-7. doi: 10.1016/j.amjcard.2012.09.027. Epub 2012 Oct 24. PMID: 23102885
Sharifi M, Berger J, Beeston P, Bay C, Vajo Z, Javadpoor S; “PEAPETT” investigators. Pulseless electrical activity in pulmonary embolism treated with thrombolysis (from the “PEAPETT” study). Am J Emerg Med. 2016 Oct;34(10):1963-1967. doi: 10.1016/j.ajem.2016.06.094. Epub 2016 Jun 30. PMID: 27422214
Summerfield DT, Desai H, Levitov A, Grooms DA, Marik PE. Inhaled nitric oxide as salvage therapy in massive pulmonary embolism: a case series. Respir Care. 2012 Mar;57(3):444-8. doi: 10.4187/respcare.01373. Epub 2011 Oct 12. PMID: 22005573
Szold O, Khoury W, Biderman P, Klausner JM, Halpern P, Weinbroum AA. Inhaled nitric oxide improves pulmonary functions following massive pulmonary embolism: a report of four patients and review of the literature. Lung. 2006 Jan-Feb;184(1):1-5. doi: 10.1007/s00408-005-2550-7. PMID: 16598645
Tapson VF, Friedman O. Systemic Thrombolysis for Pulmonary Embolism: Who and How. Tech Vasc Interv Radiol. 2017 Sep;20(3):162-174. doi: 10.1053/j.tvir.2017.07.005. Epub 2017 Jul 5. PMID: 29029710
Tapson VF, Sterling K, Jones N, Elder M, Tripathy U, Brower J, Maholic RL, Ross CB, Natarajan K, Fong P, Greenspon L, Tamaddon H, Piracha AR, Engelhardt T, Katopodis J, Marques V, Sharp ASP, Piazza G, Goldhaber SZ. A Randomized Trial of the Optimum Duration of Acoustic Pulse Thrombolysis Procedure in Acute Intermediate-Risk Pulmonary Embolism: The OPTALYSE PE Trial. JACC Cardiovasc Interv. 2018 Jul 23;11(14):1401-1410. doi: 10.1016/j.jcin.2018.04.008. PMID: 30025734
Thrombosis Canada. Pulmonary Embolism (PE): Treatment. 2023. Available at: https://thrombosiscanada.ca/hcp/practice/clinical_guides?language=en-ca&guideID=44
Tu T, Toma C, Tapson VF, Adams C, Jaber WA, Silver M, Khandhar S, Amin R, Weinberg M, Engelhardt T, Hunter M, Holmes D, Hoots G, Hamdalla H, Maholic RL, Lilly SM, Ouriel K, Rosenfield K; FLARE Investigators. A Prospective, Single-Arm, Multicenter Trial of Catheter-Directed Mechanical Thrombectomy for Intermediate-Risk Acute Pulmonary Embolism: The FLARE Study. JACC Cardiovasc Interv. 2019 May 13;12(9):859-869. doi: 10.1016/j.jcin.2018.12.022. PMID: 31072507
Vanni S, Viviani G, Baioni M, Pepe G, Nazerian P, Socci F, Bartolucci M, Bartolini M, Grifoni S. Prognostic value of plasma lactate levels among patients with acute pulmonary embolism: the thrombo-embolism lactate outcome study. Ann Emerg Med. 2013 Mar;61(3):330-8. doi: 10.1016/j.annemergmed.2012.10.022. Epub 2013 Jan 7. PMID: 23306454
Wan S, Quinlan DJ, Agnelli G, Eikelboom JW. Thrombolysis compared with heparin for the initial treatment of pulmonary embolism: a meta-analysis of the randomized controlled trials. Circulation. 2004 Aug 10;110(6):744-9. doi: 10.1161/01.CIR.0000137826.09715.9C. Epub 2004 Jul 19. PMID: 15262836
Wang C, Zhai Z, Yang Y, Wu Q, Cheng Z, Liang L, Dai H, Huang K, Lu W, Zhang Z, Cheng X, Shen YH; China Venous Thromboembolism (VTE) Study Group. Efficacy and safety of low dose recombinant tissue-type plasminogen activator for the treatment of acute pulmonary thromboembolism: a randomized, multicenter, controlled trial. Chest. 2010 Feb;137(2):254-62. doi: 10.1378/chest.09-0765. Epub 2009 Sep 9. PMID: 19741062
Weinberg A, Tapson VF, Ramzy D. Massive Pulmonary Embolism: Extracorporeal Membrane Oxygenation and Surgical Pulmonary Embolectomy. Semin Respir Crit Care Med. 2017 Feb;38(1):66-72. doi: 10.1055/s-0036-1597559. Epub 2017 Feb 16. PMID: 28208200
Wible BC, Buckley JR, Cho KH, Bunte MC, Saucier NA, Borsa JJ. Safety and Efficacy of Acute Pulmonary Embolism Treated via Large-Bore Aspiration Mechanical Thrombectomy Using the Inari FlowTriever Device. J Vasc Interv Radiol. 2019 Sep;30(9):1370-1375. doi: 10.1016/j.jvir.2019.05.024. Epub 2019 Jul 30. PMID: 31375449
Wright C, Goldenberg I, Schleede S, McNitt S, Gosev I, Elbadawi A, Pietropaoli A, Barrus B, Chen YL, Mazzillo J, Acquisto NM, Van Galen J, Hamer A, Marinescu M, Delehanty J, Cameron SJ. Effect of a Multidisciplinary Pulmonary Embolism Response Team on Patient Mortality. Am J Cardiol. 2021 Dec 15;161:102-107. doi: 10.1016/j.amjcard.2021.08.066. PMID: 34794606
Xu Q, Huang K, Zhai Z, Yang Y, Wang J, Wang C. Initial thrombolysis treatment compared with anticoagulation for acute intermediate-risk pulmonary embolism: a meta-analysis. J Thorac Dis. 2015 May;7(5):810-21. doi: 10.3978/j.issn.2072-1439.2015.04.51. PMID: 26101636
Yilmaz ES, Uzun O. Low-dose thrombolysis for submassive pulmonary embolism. J Investig Med. 2021 Dec;69(8):1439-1446. doi: 10.1136/jim-2021-001816. Epub 2021 Jun 7. PMID: 34099544
Zhang Z, Zhai ZG, Liang LR, Liu FF, Yang YH, Wang C. Lower dosage of recombinant tissue-type plasminogen activator (rt-PA) in the treatment of acute pulmonary embolism: a systematic review and meta-analysis. Thromb Res. 2014 Mar;133(3):357-63. doi: 10.1016/j.thromres.2013.12.026. Epub 2013 Dec 23. PMID: 24412030





