Today, I review, link to, and excerpt from Patterns of ischemic posterior circulation strokes: A clinical, anatomical, and radiological review [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Int J Stroke. 2022 Aug;17(7):714-722. doi: 10.1177/17474930211046758. Epub 2021 Sep 28.
There are 149 similar articles in PubMed.
The above article has been cited by 23 articles inPubMed.
All that follows is from the above resource.
- Abstract
- Stroke mechanisms and general clinical features
- Methods
- Vertebral artery strokes
- Basilar artery strokes
- Cerebellar artery strokes
- Posterior cerebral artery strokes
- Prognosis in posterior circulation strokes
- Imaging basics of PC strokes
- Supplemental Material
- Acknowledgements
- Footnotes
- References
- Associated Data
Abstract
Background: Posterior circulation and anterior circulation strokes share many clinical, pathogenetic and radiological features, although some clinical signs are highly specific to posterior circulation strokes. Arterial stenosis and occlusions occur in significant numbers in both acute posterior circulation and anterior circulation strokes, making them good candidates for endovascular treatment. Among posterior circulation strokes, basilar artery occlusions stand out because of the diagnostic and acute treatment challenges.
Methods: We reviewed the literature on clinical stroke syndromes and neuroimaging findings and systematically describe for each anatomical site of stroke the detailed clinical and radiological information (anatomical representation, diffusion weighted imaging and angiographic sequences). The principles of neuroimaging of posterior circulation strokes and the prognosis for each stroke localization are also discussed.
Review summary: Stroke syndromes in the territories of the vertebral, basilar, cerebellar, and posterior cerebral arteries are presented. Features typical of posterior circulation strokes are highlighted, including patterns of basilar artery occlusions. Clinical severity and prognosis of posterior circulation strokes are highly variable, and given that they are more difficult to detect on CT-based neuroimaging, magnetic resonance imaging is the technique of choice in suspected posterior circulation strokes. Rapid identification of arterial occlusion patterns may provide prognostic information and support acute revascularization decisions.
Conclusions: Posterior circulation stroke syndromes tightly reflect lesion localization and arterial occlusion patterns. Although many clinical and pathogenetic features are similar to anterior circulation strokes, notable differences exist in terms of clinical presentation, stroke mechanism, prognosis, and response to acute recanalization.
Keywords: Basilar artery; Ischemic stroke; Magnetic Resonance Imaging; Prognosis; Vertebrobasilar insufficiency.
Stroke mechanisms and general clinical features
Posterior circulation (PC) and anterior circulation (AC) strokes share many clinical and pathophysiological features, but there are notable differences mainly related to their respective cerebrovascular anatomy and brainstem functions. Whereas age and cerebrovascular risk factors seem similar, male sex appears more frequent in PC strokes.1
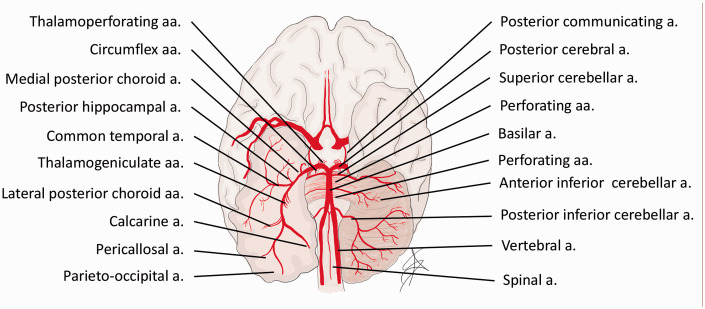
Some clinical signs are highly specific to PC strokes because of the unique brainstem functions and vascularization (Figure 1).
Figure 1.
Anatomy and vascularization of the vertebrobasilar system.
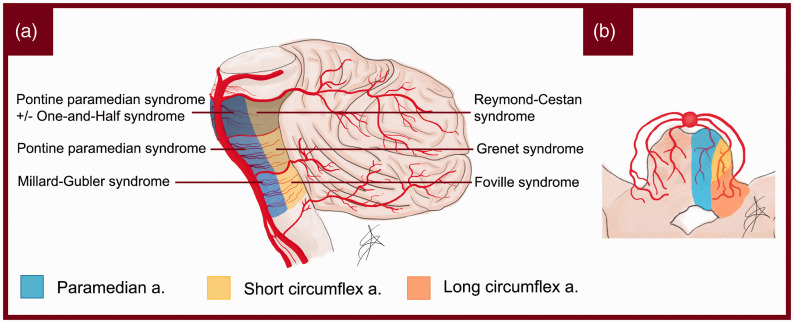
The basilar artery, in fact, gives origin to a peculiar network of perforating and circumferential arteries, which systematically repeats itself at each anatomical level of the brainstem (Figure 2).
Figure 2.
(a) Schematization of pontine syndromes. (b) Pattern of perforating branches in the pons.
Oculomotor deficits such as unilateral palsy of eye movements, internuclear ophthalmoplegia, and skew deviation are pathognomonic for brainstem locations of stroke. 1 This is also true for vertical nystagmus, up- or down-gaze palsy and conjugate gaze paresis to one side. Crossed syndromes and bilateral long tract signs are highly specific because of the bilateral supply of the basilar artery to the posterior fossa structures, and the frequent crossing of fiber tracts in the brainstem. Central vestibular symptoms and signs such as nausea, vertigo, conjugate nystagmus in any direction, gait and hemi-ataxia are also characteristic of brainstem and cerebellar strokes.2,3 Lesions of the lower brainstem and cerebellum commonly cause true vertigo and conjugate horizontal/rotatory nystagmus, whereas strokes of the upper brainstem and cerebellum cause unsteadiness and gait ataxia. Infrequent but moderately specific signs are decreased level of consciousness and amnestic syndromes, which are often missed in the acute phase or mistaken for confusional state.
Hemispheric symptoms or signs such as aphasia, hemineglect, or conjugate eye deviation are rare in PC strokes, but may still occur due to the involvement of the thalamus; in this case, an important unilateral posterior cerebral artery (PCA) stroke can even clinically mimic an AC stroke. 3 Exceptionally, cerebellar stroke can also lead to cognitive dysfunction, related to bidirectional connections with the cortex (“diaschisis”). 4
Contrary to general belief, dysarthria1,3 and homonymous visual field deficits 1 do not seem to be more frequent in PC than in AC strokes. However, PCA strokes more often cause isolated field deficits than middle cerebral artery (MCA) strokes.
The presence of multilevel lesions is peculiar to PC strokes. Symptoms may in fact be explained by the presence of two or more concomitant lesions. This feature is typical of PC strokes and is explained by the fact that the vertebrobasilar system stretches along multiple structures of the posterior fossa.
All mechanisms accounting for ischemic AC strokes also occur in the PC, and there are no consistent differences in their frequencies.1,5 In the largest comparative study, lacunar strokes seemed more frequent in the PC, 1 which could be due to the high density of long tracts and cranial nerve structures in the brainstem. Therefore, small PC strokes may be more expressive than in the AC, which is less densely packed with neuronal and axonal structures.
For the same reason, acute neuroimaging (including MRI) may not show a clinical brainstem stroke (i.e. false-negative imaging). A negative MRI in face of a vascular brainstem syndrome should not preclude a stroke diagnosis. This is particularly true for patients with acute symptom onset, absence of alternative explanations, and cerebrovascular risk factors.
Finally, most studies show a lower initial stroke severity in PC strokes. This may be due to the more frequent lacunar strokes or an underrepresentation of clinical PC deficits (ataxia, gait, oculomotor signs, amnesia) in the NIHSS scale. 6
The aim of this review is to present systematically the clinical–radiological correlations in PC strokes through the description of typical symptoms, anatomical drawings, and MRI-based examples.
Methods
We reviewed the literature for clinical stroke syndromes, anatomical vascular territories, and stroke patterns described from neuroimaging and autopsies. Examples of neuroradiological images were identified from the Acute STroke Registry and Analysis of Lausanne (ASTRAL). The first author realized anatomical drawings of territories using a Wacom Intuos© (Kazo, Japan) graphic tablet and Adobe Photoshop© (California, USA) software.
Vertebral artery strokes
Anatomy of the vertebral arteries
Vertebral arteries (VAs) constitute an essential part of the vertebrobasilar system, supplying almost 30% of the entire cerebral blood flow. 7 Anatomically, each VA can be divided into an extracranial portion (V1–V3) and an intracranial portion (V4) (Figure 1).
Figure 1.
Anatomy and vascularization of the vertebrobasilar system.
Vertebral artery hypoplasia, defined as an artery with a diameter of less than 2 mm, is observed in approximately 15% of cases. 8 The main branches supplied by the vertebral arteries originate from V4: the anterior spinal artery, which vascularizes the anterior surface of the medulla and the spinal cord; and the posterior inferior cerebellar artery (PICA), which generally supplies the ipsilateral lower medulla, posterior-inferior cerebellum and inferior vermis. The size of the PICA varies and may be inversely proportional to the size of the ipsilateral anterior inferior cerebellar artery (AICA). 9
Clinical presentation of vertebral artery strokes
VA stroke represents the most common kind of PC stroke and usually causes a bulbar lateral syndrome, historically known as Wallenberg syndrome (Supplementary Figure 1). The entity and clinical picture strongly depend on the vasculature diversification, with the lateral bulbar region being mainly supplied by the VA and PICA (Supplementary Figure 1).
A branch of the VA, the posterior spinal artery, often overlaps with the PICA to vascularize the most dorsal segment of the medulla. 10 This peculiar distinction reflects the clinical picture, with more or less extensive impairment of the lateral bulb at the rostro-caudal level. A severe infarct with extensive ischemic damage can cause a hemibulb syndrome, also known as Babinski-Nageotte syndrome (Supplementary Figure 1). In some cases, the clinical picture can be worsened by the appearance of a central alveolar hypoventilation syndrome known as Ondine syndrome. 11 This syndrome is characterized by failure of the breathing mechanisms during sleep, resulting in prolonged apneas.
Anterior spinal artery stroke causes median medullary syndrome, historically known as Dejerine syndrome (Supplementary Figure 1). A crossed syndrome results as a consequence of a lesion in the corticospinal tract above the decussation, a lesion of the medial lemniscus or a lesion of the fibers originating from the VIII nucleus. In addition, occlusion of this artery may result in an infarction of the anterior upper part of the cervical spinal cord, resulting in tetraparesis.
Basilar artery strokes
Anatomy of the basilar artery
The basilar artery (BA) originates from the conjunction of the two VAs at the intracranial level. Anatomically, it can be divided into three segments: proximal, middle, and distal. This division is reflected in the perforating branches originating from the BA, supplying the entire pons. We find the caudal group, from the juncture of the VAs to the anterior inferior cerebellar artery (AICA), the medium group, between the AICA and the posterolateral artery, and the rostral group from the posterolateral artery upwards (Figure 2(a)).
Figure 2
(a) Schematization of pontine syndromes. (b) Pattern of perforating branches in the pons.
Each group then gives origin to the perforating branches that enter the brainstem medio-laterally as the paramedian, short circumferential and long circumferential branches (Figure 2(b)). 12Clinical presentation of non-occlusive BA territory strokes
The clinical presentation of non-occlusive pontine strokes strongly depends on the pattern of involvement of the perforating branches. Excluding the lateral territory of the pons, which is supplied mainly by the AICA, we can schematically divide the pons into six areas (Figure 2(a)): a medial-ventral group supported primarily by the paramedian branches of the BA and a tegmental or dorsal group supported partially by the paramedian but mostly by the circumflex branches. Each of these areas can be subdivided in caudal, mid, and rostral groups according to the craniocaudal distribution.
Detailed clinical, MRI, and angiographic presentations according to the site of lesion are provided in Supplementary Figure 2.
Clinical presentation of BA occlusions
BA ischemic strokes are caused by large-artery atheroembolism in about two-thirds of cases, which may explain their frequently progressive onset when compared to other strokes. 13 Cardioembolisms account for one quarter of cases, and small vessel disease the rest. A few rare strokes are caused by arterial dissection. 14
Occlusive thrombi can affect either the proximal, mid, or distal portion of the BA, resulting in very heterogeneous symptoms according to the extent of ischemic infarction. The rapidity of occlusion and the contribution of the collateral circulation account for a large part of this variability.
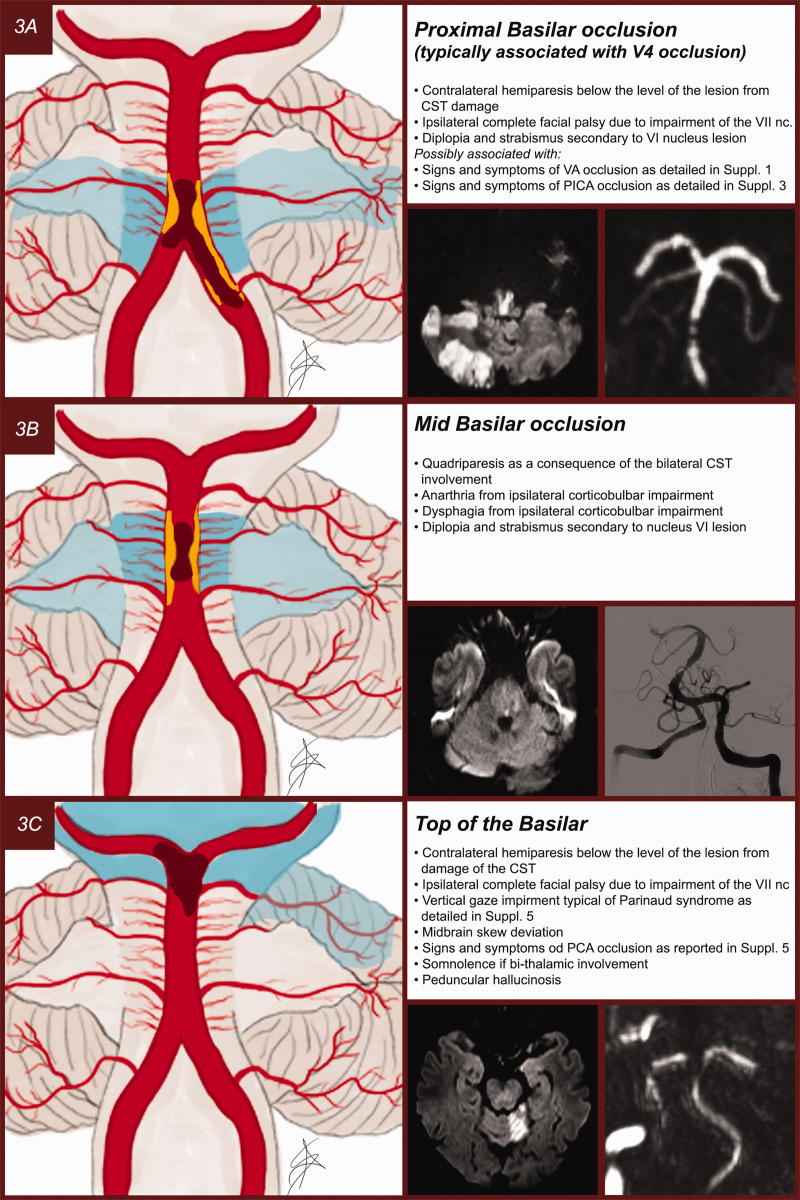
Occlusions involving the proximal and mid BA (Figure 3(a) and (b)) are for the most part caused by an atherothrombotic event and typically appear in combination with vertebral artery lesions. 15 They usually result in large pontine infarcts with a combination of signs and symptoms that can be traced to the occlusion at the origin of the perforating branches as shown in Figures 2 and 3. In such lesions, vascularization of the distal BA and PCAs largely depends on the activation of a retrograde flow provided by the posterior communicating arteries (PComs). Symptoms range from milder cases of unilateral and crossed pontine syndromes to the worst-case scenario of bilateral involvement of pontine structures resulting in a “locked-in” syndrome.
Figure 3.
(a) Proximal BA occlusion usually secondary to atheromathosis of the terminal portion of the VA. (b) Mid BA occlusion usually secondary to atheromatosis of the BA. (c) Top of the basilar occlusion usually secondary to cardioembolism.
Occlusions involving the distal BA are more often cardioembolic in nature. 15 The resulting top of the basilar syndrome (Figure 3(c)) 16 may present with a wide range of symptoms, depending mainly on the length and position of the clot and on collateral flow provided by the PComs to vascularize the PCA territory. It may present with a sudden decreased level of consciousness due to the usually bilateral involvement of either the reticular formation or of the thalamus. Other features may consist of behavioral change and quadriplegia, followed by ataxia, oculomotor impairment seen as either vertical and/or horizontal gaze palsy, impairment of the oculocephalic reflex, pupillary abnormalities, visual deficits, and sensory dysfunction. 17
Cerebellar artery strokes
Anatomy of the cerebellar arteries
The cerebellum is composed of a midline vermis and two hemispheres. Blood is supplied by three pairs of arteries: the PICA, AICA, and superior cerebellar artery (SCA) (Supplementary Figure 3).
The AICA originates from the middle segment of the BA and vascularizes the antero-inferior cerebellum. Its collateral branch, the internal auditory artery, supplies the vestibulocochlear nerve and inner ear. The SCA emerges from the distal segment of the BA. It splits into medial and lateral branches, which vascularizes the superior cerebellum and superior vermis. The cerebellar vascularization often presents variations such as a common trunk of the AICA and PICA, or bilateral vascularization by a unique artery. 18
Clinical presentation of cerebellar artery strokes
Infarctions limited to the cerebellum present, in order of frequency, vertigo and dizziness, nausea and vomiting, gait unsteadiness, headache, dysarthria, and neurological signs such as limb or trunk ataxia, dysarthria or nystagmus, often absent or subtle. 19 Upper cerebellar lesions generally present dysarthria, and lower, mostly vertigo, nausea, and vomiting. Cognitive symptoms (“diaschisis”) are possible but rare. 4
The PICA is the territory frequently involved in cerebellar strokes, followed by the SCA and AICA. Approximately one third of cerebellar strokes involve multiple vascular territories, while 20–30% of cases present as borderzone strokes. 20
Posterior cerebral artery strokes
Anatomy of the PCA
The BA divides into two PCA terminal branches at the level of the ponto-mesencephalic junction. Each PCA is split into four segments: P1, from the termination of the BA to the origin of the PCom; P2, between the PComs and the posterior margin of the midbrain; P3, from the pulvinar to the anterior limit of the calcarine fissure and P4, the cortical segment within the calcarine fissure becoming the calcarine artery (Supplementary Figure 4). 21
The PCAs supply blood to the rostral midbrain, the medial and posterolateral regions of the thalamus, the hippocampus and the occipital, temporal and partially the parietal lobes. Historically, we distinguish two main territories of vascular supply: a proximal or deep PCA territory, including the thalamus, and a distal or superficial PCA territory, including the hemispheric occipital and temporo-parietal lobes. 22
Clinical presentation of PCA strokes
Infarctions of the PCA territory are usually associated with homonymous visual field defects, especially hemianopia. However, multiple additional symptoms and signs are often present, such as sensory and motor abnormalities and cognitive and neuropsychological deficits.22–24 These infarcts can simulate MCA strokes, particularly in the presence of significant motor deficits. 25 The main types of PCA infarctions and their clinical-radiological correlations are summarized in Supplementary Figure 5.
Up to 40% of PCA strokes have concomitant infarcts elsewhere in the PC and sometimes in the carotid territory. 24 Among patients with isolated PCA occlusion, the involvement of deep structures varies between 34 and 64% across studies, with the ventrolateral thalamus being the most commonly affected structure. 24
Prognosis in posterior circulation strokes
There is little data on the overall prognosis of PC strokes; the largest analysis found comparable long-term outcomes to those of AC strokes after adjustment for the usual prognostic factors. 1 PC strokes arriving later than 4.5 h after last proof of good health seem to have a worse prognosis than late arriving AC strokes. 26
Because PC strokes have been underrepresented in randomized trials, their response to acute revascularization is less well known. Whereas the response to thrombolysis seems similar to AC strokes,27,28 an effect of EVT is not yet proven.29,30
Prognosis after VA strokes is poorly known, but small studies have shown a high stroke recurrence risk in demonstrated bilateral VA strokes. 31
Observational studies on cerebellar infarctions reported a rate of functional independence at three months of 69% and a mortality rate of 7%. 32 The prognosis mainly depends on the severity of the associated brainstem lesions and on the initial threat of ischemic mass effect. The latter occurs in 10–20% of cases and nearly always involves the PICA territory. 33
Prognosis of BAOs stands out because of the several clinical challenges. Firstly, they may be initially missed clinically as an acutely decreased level of consciousness and absence of lateralizing signs are rather rare in acute stroke. 34 Secondly, BAOs have one of the most unfavorable prognoses of all strokes unless early recanalization treatment is associated with rapid clinical improvement. Finally, acute EVT of BAOs still lacks an unequivocal proof of effectiveness.29,30
Clinical outcome after a PCA stroke is critically related to the involvement of the thalamic and brainstem structures, but also the contralateral PCA. PCA strokes are usually regarded as less troublesome than anterior strokes, primarily due to the lower incidence of motor deficits, less mass effect, and lower mortality. 35 However, in the long-term, patients with thalamic strokes may be affected by sensory-related sequelae or cognitive and neuropsychiatric disturbances. 36 Similarly, in patients with superficial PCA strokes, visual field defects and neuropsychological deficits may remain as disabling consequences. There are no controlled trials of revascularization treatments of the PCA. The largest retrospective study indicated a better cognitive and visual outcome with effective recanalization treatments like EVT. 37
Imaging basics of PC strokes
All patients with a suspicion of stroke require urgent brain imaging to confirm the diagnosis, to assess the extent of ischemic damage and to detect the level of vascular occlusion in order to begin adequate therapy. Imaging can also add prognostic information. Imaging can be done using either computed tomography (CT) or better still, magnetic resonance imaging (MRI) given its higher sensitivity for detecting acute ischemic lesions. MRI is, however, subject to contraindications such as implanted devices or claustrophobia.
Non-contrast CT (NCCT) allows a reliable exclusion of hemorrhagic stroke. However, it has very low sensitivity for diagnosing AIS, mainly due to the smaller nature of the lesions and to the skull base-related beam hardening. If lesions are present, the extension of early ischemic changes on CT assessed by the PC Alberta Stroke Program Early CT score (pc-ASPECTs), has demonstrated independent predictive value of patients’ outcomes. 38 The analysis of computed tomography angiography (CTA) source imaging significantly increases the performance of CT for detecting ischemic changes from 21–46% to 27–65%39,40 and improves the prognostic value of pc-ASPECTs.39,41 Similarly, adding CT perfusion (CTP) to NCCT and CTA increases the sensitivity and helps to identify patients with predicted worse outcomes. 42
MRI-based imaging
Non-contrast MRI with diffusion weighted imaging (DWI) is much more sensitive than NCCT for diagnosing AIS, in particular in the brainstem where lesions are often small. 43 The pc-ASPECTs may be performed on DWI and also helps in evaluating patient prognosis. 44 Still, DWI on the PC may be negative on initial imaging. 45 In patients initially presenting with acute dizziness/vertigo, PC stroke with negative DWI principally corresponded to ischemia of the medulla and pons followed by ischemia of the cerebellum and midbrain. 46 One can assume that most negative DWI corresponds to focal infarcts due to small-vessel disease, and some authors reported that the time course of diffusion imaging in brainstem infarct is more than twice as slow as in AC infarct. 47 Therefore, repeating DWI-imaging in the subacute phase may be useful if the cause of symptoms remains uncertain.
46.Choi JH, Oh EH, Park MG, et al. Early MRI-negative posterior circulation stroke presenting as acute dizziness. J Neurol 2018; 265: 2993–3000. [DOI] [PubMed] [Google Scholar][Ref list]
47.Axer H, Grassel D, Bramer D, et al. Time course of diffusion imaging in acute brainstem infarcts. J Magn Reson Imaging 2007; 26: 905–912. [DOI] [PubMed] [Google Scholar][Ref list]
Arterial imaging
Beyond detection of cerebral ischemic changes, neuroimaging is required to demonstrate pathologies of the vertebrobasilar cervical and intracranial arteries. This imaging should be performed in the hyperacute phase using CTA or MRA. To detect vertebral artery stenosis, MRA demonstrated higher sensitivity than CTA or Doppler ultrasound, along with higher specificity. 48 Moreover, high-resolution two-dimensional and three-dimensional non-contrast fat-sat spin echo T1-weighted sequences may help visualize cervical and intracranial stenosis, 49 intraplaque hemorrhage, 50 vertebral wall hematoma 51 as well as determine dissection age. 52 Contrast-enhanced 3D-BB sequences additionally help to differentiate common cervical arteriopathies such as dissection, atherosclerosis, and vasculitis with an excellent inter-reader reproducibility. 53
For BAO, several radiological scores have shown independent prognostic value: the posterior circulation-collateral score (PC-CS), the PC vascular score (pc-CTA), the basilar artery score (BATMAN), and PComs patency score on CTA, in addition to the hyperintense basilar artery sign score on FLAIR and the potential feeding artery score on MRA.54–56 Still, harmonization and external validation of these scores, and development of a PC occlusion score beyond BAOs are needed.