
See also Update on Diagnosis and Management of Kawasaki Disease: A Scientific Statement From the American Heart Association [PubMed Abstract] [Full-Text HTML] [Full-Text PDF]. Circulation. 2024 Dec 3;150(23):e481-e500. doi: 10.1161/CIR.0000000000001295. Epub 2024 Nov 13.
Erratum in
Abstract
Kawasaki disease (KD), an acute self-limited febrile illness that primarily affects children <5 years old, is the leading cause of acquired heart disease in developed countries, with the potential of leading to coronary artery dilation and coronary artery aneurysms in 25% of untreated patients. This update summarizes relevant clinical data published since the 2017 American Heart Association scientific statement on KD related to diagnosis, cardiac imaging in acute KD treatment, and long-term management. Criteria defining North American patients at high risk for developing coronary artery aneurysms who may benefit from more intensive initial treatment have been published. Advances in cardiovascular imaging have improved the ability to identify coronary artery stenosis in patients with KD, yet knowledge gaps remain regarding optimal frequency of serial imaging and the best imaging modality to identify those at risk for inducible myocardial ischemia. Recent data have advanced the understanding of safety and dosing for several anti-inflammatory therapies in KD. New anticoagulation medication, myocardial infarction management, transition of health care for patients with KD, and future directions in research are discussed.
Keywords: AHA Scientific Statements; coronary aneurysm; diagnosis; heart disease; immunoglobulins, intravenous; mucocutaneous lymph node syndrome; thrombosis; vasculitis.
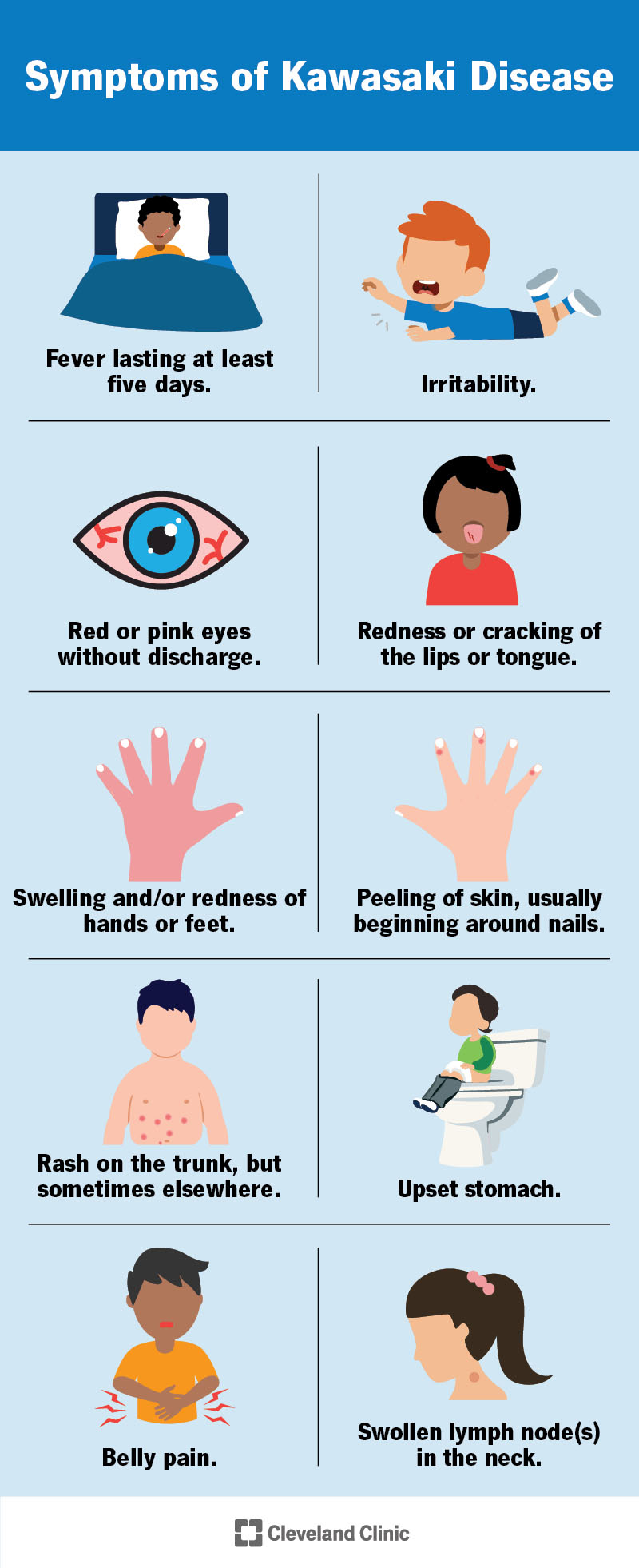
Information on Kawasaki Disease from Cleveland Clinic:
Kawasaki disease has many symptoms, like fever, red tongue, rash and belly pain.
Today, I review, link to, and excerpt from StatPearls‘ Kawasaki Disease. Angeline M.Owens; Michael C. Plewa. Last Update: June 26, 2023.
All that follows is from the above resource.
Introduction
Kawasaki disease (KD), also known by the name mucocutaneous lymph node syndrome, is an acute, self-limited medium vessel vasculitis that has a predilection for the coronary arteries.[1] It is the leading cause of acquired heart disease in developed nations and is slowly bypassing rheumatic heart disease in developing countries.[2][3]
Etiology
The etiology of Kawasaki disease (KD) is still not known and may be related to a wind-borne or water-borne pathogen. However, in recent years there have been studies that have shown certain genetic markers (such as HLA-B51 and HLA-Bw22j2 serotypes, chemokine receptor gene-cluster CCR2-CCR5 haplotypes and FCGR3A polymorphism of the IgG receptor IIIa) show a predisposition to the disease. In fact, siblings are 10-20 times more likely to develop the disease when compared to the general population.[1][3][4] There is no evidence to suggest that the disease passes from person to person. Multiple organisms of bacterial and viral origin have are under suspicion as a cause, but to date, no single agent has been identified as the leading cause.[1] However, there has been evidence showing over 40% of children diagnosed with KD have tested positive for viral respiratory pathogens.[5]
EpidemiologyThis disease is most common in children younger than five years of age, but it can present at any age, even in adults.[4] There is a slight male predominance (male to female = 1.5 to 1).[2][6][4] Boys are also more likely to suffer from complications and death.[3] It is rare to see Kawasaki disease in children less than 4 months, possibly pointing to protection from maternal antibodies.[1] It is most commonly seen in children of Asian descent, particularly Japanese, and is least common in Caucasian children.[1] There also appears to be a higher prevalence of the disease in the winter and spring months.[1][3][4] Incidence varies from 10 to 20 in 100,000 children aged < 5 years in the U.S. and Canada to 50 to 250 in 100,000 in Japan, Taiwan or Korea.
Pathophysiology
An agent, most likely infectious, enters via the respiratory tract and starts a response that activates lymphocytes, cytokines, and proteinases, specifically tumor necrosis factor alpha (TNF-a), Interleukin 1, 4 and 6 and matrix metalloproteinases (MMP3 and MMP9)[7]. Oligoclonal IgA plasma cells are believed to play a crucial role in the cascade leading to coronary arteritis and are also prominent in the respiratory tract which is why the thinking is that a respiratory infection triggers the disease process.[1] This activation causes myocarditis and arteritis and, from fibrinoid necrosis of the internal elastic lamina, the development of a weak spot in the vessel wall that predisposes it to an aneurysmal formation from neutrophil invasion.[1] Atypical activation of monocytes and macrophages is considered the cause of these vascular lesions, which is unique to Kawasaki disease and is suggestive that an innate immune response triggers this process.[6][7][8] Over weeks and months, wall thickening of the coronary aneurysms can lead to stenosis and thrombus formation which can result in myocardial infarction (MI), rupture, ischemia-related dysrhythmias or death. The greatest risk of these cardiac complications is during the period of thrombocytosis. Small coronary aneurysms may resolve in 60% of cases in the later convalescent phase when inflammatory markers return to normal.
Histopathology
A biopsy is rarely performed and is not necessary to make a diagnosis. Findings early in the disease show destruction of the media of vessels by neutrophils.[8] Coronary arteritis characteristically presents with granulomatous inflammation that develops 6-8 days into the illness and is present across all layers of the vessel.[4][9] As the disease progresses, the infiltration gets replaced by lymphocytes, monocytes, and fibroblasts which lead to arterial remodeling.[8] Both light and electron microscopy show cytoplasmic inclusion bodies containing RNA in 85% of acute and late-stage fatalities.[10]
History and Physical
These children will present with multiple days of fever and generalized malaise. On physical exam, one will often find one or more of the diagnostic criteria listed below. It is important to get a full history because meeting any of the diagnostic criteria at any point during the illness count toward the diagnosis of Kawasaki disease, even if not present at the time of evaluation. There are three principal stages of the disease process: acute, subacute, and convalescent.[11][12] The acute phase consists of an abrupt onset of high fever that lasts 1 to 2 weeks but can last up to 3 to 4 weeks if left untreated. During the acute phase rash, conjunctivitis and myocarditis occur. The subacute phase begins when the fever subsides and lasts into weeks 4 to 6 of the disease course. The patient will have desquamation of the hands, thrombocytosis, and the development of coronary artery aneurysms. The convalescent phase is when the clinical signs of the illness cease, which is typically within 3 months from the initial onset of the disease. Cardiac abnormalities can still be apparent in this stage; however, new aneurysms after 8 weeks of illness are unusual.[13]
A variety of less common manifestations include abdominal pain, vomiting or diarrhea in 20%; hepatitis; parotitis; intussusception; joint pain in between 15-50%, especially the larger weight-bearing joints [1]; headache, irritability, seizure, aseptic meningitis; rhinorrhea and cough in 20-30%; aortic aneurysms; valvular insufficiency; epididymitis, orchitis or urethritis. Purulent conjunctivitis or exudative pharyngitis findings would each suggest a diagnosis other than KD.
In 2014, the American Heart Association (AHA) published the criteria needed to establish a diagnosis.[1] However, it is important to note that children who fall short of the full criteria but have cardiac abnormalities on echocardiogram meet the diagnosis of KD.[1] The patient must have fevers for five or more days, with at least four of the following criteria (either all at once or over a series of days):
Patients will typically have a patchy generalized macular erythematous rash over the trunk and extremities that appears within 5 days of the fever, and mocks a viral exanthem or drug eruption, but will lack pruritus.[1][3][14] Patients will also typically have peeling of the skin in the periungual area that starts about 2 to 3 weeks after onset of fever, which is characteristic of KD.[1] Nail changes, typically transverse depressions (Beau’s lines)*, are seen in over 75% of patients with the disease that appear about 5 to 8 days after the onset of the fever and can last 2 to 4 weeks.[1][3][6]
*Images of Beau’s Lines from Skinsight:





Resuming Kawasaki Disease from StatPearls:
Evaluation
The diagnosis of Kawasaki disease is clinical. You can use the mnemonic “Warm CREAM” or “FEBRILE” to help remember the criteria (see Table). The fever is the most consistent presentation, is minimally responsive to antipyretics, and typically remains higher than 38.5 degrees Celsius.[1][6] A conjunctival injection can also present with photophobia and can correlate with uveitis in about 65% of patients.[6] All of these symptoms tend to present sequentially, which indicates the diagnosis of KD over other disease processes on the differential.[2] The diagnosis of complete KD should be made in the acute phase of the process.[3]
Table: Warm CREAM and FEBRILE Mnemonics for KD Criteria
Warm = Fever for > 5 days
Incomplete Kawasaki disease should be a consideration in children with fevers of five or more days and two or three of the major criteria. It is more common in younger infants and older children.[1][2][4] Therefore, if an infant younger than 6 months has a prolonged fever of over 7 days, it is important to get an echocardiogram to rule out KD.[2][4] The AHA has created an algorithm for these patients which involves lab studies and an echocardiogram to make the diagnosis.[3] If a C-reactive protein (CRP) is < 30 mg/l and erythrocyte sedimentation rate (ESR) < 40 mm/hr, then follow the patient daily; if fever resolves and peeling of the skin occurs, get an echocardiogram and treat if aneurysms detected. If the CRP > 30 mg/l and/or ESR > 40 mm/hr, then get an echocardiogram. To meet incomplete KD criteria, initiate treatment, and obtain an echocardiogram, more than three of the following must be present[15]:
There are no other required laboratory or diagnostic imaging studies necessary after a clinical diagnosis of KD, except an echocardiogram. However, some studies may be useful in the case of incomplete disease in an attempt to help narrow the diagnosis when not meeting all of the clinical criteria. Suggested studies include complete blood count (CBC), metabolic panel, ESR, CRP, and urinalysis. Mild-moderate normocytic anemia is characteristic of the acute disease phase, while thrombocytosis is present in the subacute phase.[6] Thrombocytopenia may be present less commonly in the acute phase, but predicts a greater risk for coronary artery aneurysm (CAA), and may be associated with immune thrombocytopenic purpura (ITP), disseminated intravascular coagulation (DIC), or destruction by immunoglobulin. Hypoalbuminemia may be present and correlates with a more severe and prolonged disease course.[8] Hyperbilirubinemia and elevated liver enzymes can be caused by hepatic congestion, which in turn can lead to obstructive jaundice as well as gallbladder hydrops.[1][6][16][17] Acute phase reactants are almost always elevated. Pro-B-type natriuretic peptide (Pro-BNP) levels appear to correlate with a greater risk of coronary artery aneurysm formation and intravenous immunoglobulin (IVIG) resistance in patients younger than 3 months old.[3] Urinalysis will show sterile pyuria, which will be absent if the sample was from from bladder aspiration.[1][6] If a lumbar puncture is performed to help rule out other differentials, pleocytosis is a common finding in KD and can be misleading to a diagnosis or viral meningitis [1]. Since concomitant respiratory viral infections are common and may play a role in pathogenesis in KD, do not let a positive respiratory viral polymerase chain reaction (PCR) finding mislead away from the diagnosis of KD.
If obtained, blood cultures, stool cultures, antinuclear antibody (ANA), rheumatoid factor (RF) and anti-streptolysin O (ASO) titers would be negative in KD cases.
An echocardiogram should be performed during the acute phase of the disease to rule out coronary artery aneurysm (CAA). The proximal left anterior descending and right coronary arteries are most commonly affected.[18] Aneurysms can be fusiform, saccular, ectatic, or segmented. Aneurysms more likely to regress are fusiform, small and distal. It is also important to evaluate other parts of the heart to look for signs of aortic root dilation, decreased contractility, valvular dysfunction, and effusion. However, ultrasound is subject to operator ability and has difficulty assessing the mid and distal portion of the vessels. Because of this, the use of CTA of the coronary arteries is becoming more prominent as it can identify and quantify lesions with precision, especially those in the mid and distal segments of the vessels.[19] However, one must weigh the risks versus the benefits of radiation exposure in the pediatric population. Also, CT is limited in evaluating the lumen of vessels that have calcification present.[4] Some investigators are now using electron beam CT to assess for coronary artery calcifications as a marker for future coronary events.[20] Magnetic resonance angiography (MRA) is also an option if radiation exposure is a concern, and it is more sensitive for small lesions and intimal hyperplasia.[4] Electrocardiography (ECG) can show a prolonged PR interval, deep Q waves, low voltage, ST-T changes, and arrhythmias which are suggestive of myocardial damage and repolarization abnormalities.[4]
Cardiac stress testing for reversible ischemia has been recommended as Level A for children with KD and known CAAs.[1] Coronary angiography offers more detailed views of the coronary arteries when compared to echocardiogram, but is only of benefit in patients who have more complex coronary artery lesions to assess for stenosis.[1][4] It is recommended to delay angiography 6-12 months after the initial presentation.[1]
Treatment / Management
Treatment aims with Kawasaki disease point to minimize the risk of coronary artery aneurysm (CAA) formation, which peaks two to four weeks after illness onset, by decreasing the inflammation of the coronary arteries.[4] Supportive care is also essential. [See article for treatment details]
Differential Diagnosis
Various infections can mimic Kawasaki Disease including:
Both KD and adenovirus present with conjunctival injection, however, the important differentiation is that adenovirus causes conjunctival exudates and KD does not.[3] The differentiation of KD from lymphadenitis by observing whether the lymphadenopathy is bilateral or unilateral; Kawasaki typically presents unilaterally in over half of cases.[1][3] KD can cause retropharyngeal edema which may present concerning for possible retropharyngeal abscess (RPA). However, true RPA will have clinical symptoms and abnormal imaging, whereas KD will not.[3] Toxic shock syndrome and scarlet fever lack the ocular and joint involvement that KD has.[6]
Kawasaki disease’ presentation also overlaps with other immunologic reactions such as multiple drug hypersensitivity reactions, juvenile idiopathic arthritis, infantile polyarteritis nodosa, and systemic lupus erythematosus. These can be differentiated from KD by the absence of classic clinical criteria and by chronicity and the number of joints affected.[6][12]
Prognosis
Prognosis depends on the severity of cardiac disease. Additionally, the prognosis is better for children diagnosed between age 6 months to 9 years than those younger or older, perhaps because they are diagnosed earlier after presenting with classic findings.[35] Recurrence is uncommon but is most likely to occur in younger children who had cardiac complications from the disease during the initial episode. All KD related deaths are essentially the result of cardiac complications and typically occur 15-45 days from the onset of fever.[1]
Complications
The disease can lead to aneurysm formation, heart failure, MI, myocarditis, valvulitis, pericarditis with pericardial effusion, and rupture of the coronary arteries leading to hemopericardium and sudden death.[30] About 9% of patients will experience acute phase cardiac complications while about 3% will experience cardiac sequelae.[4] Patients with Kawasaki disease frequently have MIs while sleeping or at rest, which suggests coronary vasospasm etiology.[4] Myocardial inflammation has been seen in 50 to 70% of patients during the acute phase of the disease and has raised concern over the long-term effects that KD has on cardiac function.[1] There is documentation of mitral regurgitation and aortic regurgitation in a small number of cases in children with KD.[1] About 15-25% of untreated children will go on to develop CAAs.[1] Specific factors lead to an increased risk of coronary artery aneurysms including [1][4][5][10][11][12]:
Aneurysms are defined as vessel diameter >3mm in children younger than 5 years old and >4mm in children older than 5 years.[1] Cardiac complications later on in adulthood have been shown to be more common in those patients who had a CAA >6.0mm.[30] Giant aneurysms (>8.0mm) are likely to occlude from a thrombus within in the first year causing an MI.[19]
In those who aneurysms resolve, there will be significant thickening of the vessel leading to an increased risk of premature coronary atherosclerotic disease.[18] In a study done on adults who suffered from an MI later in life after having had a coronary artery aneurysm in childhood due to KD, there was no evidence of remaining aneurysm.[36] However, one cannot assume that just because an aneurysm resolves, that does not mean the risk of cardiac complications later in life also dissipates.[30]
Enhancing Healthcare Team Outcomes
Kawasaki disease is a rare disorder, but because of its serious effects on the coronaries, the condition is best managed by an interprofessional team. Once a child is suspected of having Kawasaki disease, the patient should be referred promptly to a cardiologist.
A cardiologist should be consulted to determine the initial and schedule of following echocardiogram studies, anticoagulation management, to determine if coronary artery angiography is necessary and for long-term follow-up and monitoring. Other specialists to consider, include an infectious disease specialist, rheumatologist, or dermatologist. Following treatment, the short-term prognosis is good, but the long-term prognosis remains unknown primarily because many children are lost to followup.
Strawberry tongue KD Image courtesy S Bhimji MD
From: Kawasaki Disease
StatPearls [Internet].Treasure Island (FL): StatPearls Publishing; 2025 Jan-.





