See also The ACG Clinical Guideline for the Diagnosis and Management of Gastroesophageal Reflux Disease [PubMed Abstract] [Full-Text HTML] [Download Full-Text PDF]. Am J Gastroenterol. 2022 Jan 1;117(1):27-56.
In this post, I link to and excerpt from The Curbsiders’ #188 GERD and Dyspepsia with Dr. Amy Oxentenko MD
DECEMBER 16, 2019 By BETH GARBITELLI
All that follows is from the above resource.
Delve into the diagnosis and management of GERD and dyspepsia with Dr. Amy Oxentenko (@AmyOxentenkoMD), Gastroenterologist and the Internal Medicine Residency Program Director, Associate Chair for the Department of Internal Medicine, and Professor of Medicine at Mayo Clinic in Rochester, MN. Our discussion features a review of the standard presentations of GERD and dyspepsia, alarm symptoms and who needs referral for endoscopy or other specialized testing (pH, impedance testing, screening for Barrett’s esophagus). Additionally, we comprehensively cover proton pump inhibitor (PPI) therapy including: choice of agent, dose, frequency, how taper, how to counsel patients about risk, what labs should be monitored and the use of adjuvant therapies like H2 blockers, antacids and sucralfate. After this episode, you will be flexing on reflux!
GERD and Dyspepsia Pearls
Risk factors for GERD include physical abnormalities (diaphragm defects, hiatal hernia), delayed stomach emptying (narcotic use, gastroparesis), obesity, and all trimesters of pregnancy. (Kellerman 2017).
Patients may be diagnosed with GERD on symptoms alone.
Patients with chest pain should be worked up for cardiac conditions before blaming reflux for their symptoms. (see question 5 in American Gastroenterological Association 2008)
Worrying symptoms with reflux include dysphagia, notable weight loss (>5% body weight) and food impaction. (American Gastroenterological Association 2008)
Patients with longstanding GERD (> 5 yrs of GERD) require assessment for Barrett’s Esophagus with an upper endoscopy. (American Gastroenterological Association 2008)
Indications continuous PPI include dilated peptic stricture, significant esophagitis (ie: has caused ulceration of the distal esophagus), and those with Barrett’s Esophagus (even if asymptomatic). (American Gastroenterological Association 2008) If a patient requires indefinite or long term PPI usage, Dr. Oxentenko suggests getting objective data to confirm the GERD diagnosis either via EGD or pH.
Be wary of starting PPI in the hospital unless patient has a clear indication, due to risks of enteric infections, per Dr. Oxentenko.
PPI can be used intermittently or for short periods of time when patients know they will experience heartburn, such as when traveling or having restaurant food —Dr. Oxentenko’s expert opinion.
May check an annual creatinine, complete blood count, and serum ferritin. Check B12 levels every five years. Magnesium levels can be checked in symptomatic patients —Dr. Oxentenko’s expert opinion.
For patients seeking to go off PPI, Dr. Oxentenko suggests tapering by taking every other day for a few weeks and then every 3rd day for a few weeks before fully discontinuing —Dr. Oxentenko’s expert opinion.
Eliminating dietary causes of heartburn is not helpful unless the patient has a clear pattern of reflux from a specific food type, per Dr. Oxentenko and AGA Guidelines.
Tobacco and alcohol reduction does not necessarily improve pH readings or GERD symptoms, despite general health benefits from cessation (Kaltenbach 2006).
H. pylori infection should also be ruled out in patients with dyspepsia via urea breath test or stool antigen test. Dr. Oxentenko prefers using stool antigen as the urea breath test can have false negatives from factors like recent antibiotic use.
Diagnosing GERD
We all have physiologic reflux, but having reflux (acid or non-acid mediated) with symptoms or side effects qualifies as GERD. The pathology involves the lower esophageal sphincter. Transient relaxation occurs throughout the day, but those with pathological GERD have more frequent transient relaxation of the lower esophageal sphincter (American Gastroenterological Association 2008; Kellerman 2017).
Risk factors for GERD include physical abnormalities (diaphragm defects, hiatal hernia), delayed stomach emptying (narcotic use, gastroparesis), obesity, and all trimesters of pregnancy (Kellerman 2017).
Most patients are diagnosed with GERD based on symptoms alone, specifically heartburn and/or regurgitation. They do not need to exist in combination. Atypical symptoms include nausea, hoarseness, and enamel loss (Richter 2018, Ranjitkar 2012). Dr. Oxentenko doesn’t routine pursue labs or advanced diagnostics (endoscopy, pH testing) in patients with typical symptoms.
Check the Heart & When to Scope
Patients with chest pain should have cardiac conditions ruled out (American Gastroenterological Association 2008). Dysphagia is an alarm symptom that implies reflux-induced strictures, malignancy, or other causes. Notable weight loss (>5% body weight) in combination with dysphagia is also worrisome (American Gastroenterological Association 2008). Food impaction can indicate eosinophilic esophagitis, which is increasingly prevalent (Moawad 2018).
Dr. Oxentenko recommends that patients who do not respond to PPI therapy undergo upper endoscopy. Early endoscopy is appropriate in older patients with a sudden onset of reflux or those with iron deficiency anemia. In such patients Dr. Oxentenko may perform endoscopy before an empiric trial of PPI.
Breaking Down Barrett’s Esophagus
Patients with longstanding GERD (> 5 yrs of GERD) require assessment for Barrett’s esophagus with an upper endoscopy (American Gastroenterological Association 2008). Patients that fit this category are generally males, >50 yrs, and may have other risk factors including smoking history, obesity, and family history of upper GI malignancy.
If the initial (index) upper endoscopy for a patient fitting the profile of Barrett’s esophagus is negative, further surveillance endoscopy is not required (Spechler 2014).
The diagnosis of Barrett’s esophagus requires both endoscopic and histologic findings. Gross endoscopic findings suggesting Barrett’s esophagus include columnar mucosa extending above the gastroesophageal junction & lining the distal esophagus. A positive biopsy shows columnar metaplasia and should be evaluated by a gastrointestinal pathologist for the presence of low grade or high grade dysplasia (Spechler 2014). Patient’s with metaplasia, but no dysplasia receive surveillance endoscopy every 3-5 years. Those with low grade dysplasia should have repeat evaluation in 6-12 months. Finally, patients with high grade dysplasia qualify for immediate endoscopic eradication (Spechler 2014).
Taming the Acids
GERD Medications
First line drugs for treating GERD include omeprazole, esomeprazole, and pantoprazole. If someone does not have a response to PPI, there is weak evidence that switching to a different type of PPI will help (Mermelstein 2018). BUT, guidelines state switching once may be worth investigating (American Gastroenterological Association, 2008).
H2 Blockers are a reasonable option depending on the frequency of reflux-related symptoms. Intermittent symptoms (ie: two or less times a week) can be managed with either antacids alone or an over-the-counter H2 blocker as needed –Dr. Oxentenko’s expert opinion.
PPI for Life?
Indications for continuous PPI therapy include peptic stricture, significant esophagitis (ie: has caused ulceration of the distal esophagus), and those with Barrett’s esophagus (even if asymptomatic) (American Gastroenterological Association 2008).
Concerns about PPI Side Effects
Many of the original studies that raised concerns about the safety of PPIs were large, retrospective, observational studies that had sick patient groups and very small hazard ratios. Dr. Oxentenko points out that these associations do not prove cause and effect.
The interaction with clopidogrel does not have as much clinical significance as previously thought (Juurlink 2009).
In a patient who needs a PPI and has no predisposing factors for osteoporosis, there is nothing that should be done differently, per Dr. Oxentenko. Ensure adequate calcium intake and bone density screening as indicated by age and risk factors, but PPI should not be avoided if needed as evidence is conflicting (Targownik 2017). If patient has osteoporosis, engage in shared decision making with the patient (Expert opinion).
Patients may be at increased risk for infectious GI complications, including C. difficile when on PPI (Trifan 2017). If someone is at risk for traveler’s diarrhea on an upcoming trip and has mild heartburn, cutting back on PPI may be helpful. Patients in the hospital with risk for C. difficile should not be started on PPI unless there is a clear indication (e.g. a bleeding ulcer), per Dr. Oxentenko.
Long term PPI use could affect B12 and iron absorption, but there has not been a population level deficiency for these associations. It is physiologically possible as an acidic milieu is required for absorption of these compounds (Vaezi 2017). PPI use may affect magnesium transport, and deficiency can be seen (Vaezi 2017).
Associations from retrospective studies have suggested that PPI use may predispose patients to chronic kidney disease, dementia, certain infections and a host of other concerns (Vaezi 2017), but Dr. Oxentenko believes the evidence is weak and does not prove causation. Further, a recent prospective, randomized trial with median three years follow up found no increased risk for infection, CKD, dementia or fractures in patients taking PPIs (Moayyedi 2019). All that being said, patients should not be prescribed PPI therapy without a clear indication.
Initial Counsel for Patients
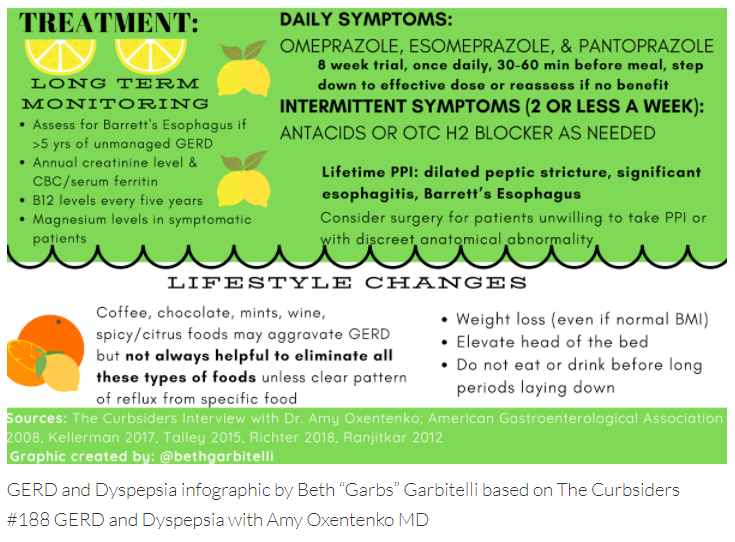
Dr. Oxentenko advises initial empiric PPI therapy for 8 weeks with follow-up afterwards to assess benefit for the patient’s symptoms. The PPI is taken once daily in the morning 30-60 minutes before a meal. If possible, step down therapy and place patient on lowest effective dose (American Gastroenterological Association 2008). Be wary of starting PPI in the hospital unless patient has a clear indication (expert opinion). If a patient requires indefinite or long term PPI usage, Dr. Oxentenko suggests getting objective data to confirm the GERD diagnosis either via EGD or pH monitoring.
PPI therapy can be used intermittently or for short periods of time when patients know they will experience heartburn, such as when traveling or having restaurant food, according to Dr. Oxentenko’s expert opinion.
Monitoring Long Term PPI Usage
Dr. Oxentenko notes that clinicians can consider checking an annual creatinine level to assess renal function, a CBC, and serum ferritin for anemia. B12 levels can be checked every five years. Magnesium levels can be checked in symptomatic patients (expert opinion).
Lifestyle modifications
Weight loss can be helpful even in patients with a normal BMI, per Dr. Oxentenko. Elevation of the head of the bed at night with wedges can be helpful for those with nocturnal symptoms. (American Gastroenterological Association 2008). Simply propping head up on pillows may not be helpful since it can put more pressure on the abdomen. Patients should not eat or drink for a few hours before bed (or even sooner, if they lay on the couch). Patients should be counseled to avoid recumbency immediately after meals.
There are foods that may aggravate symptoms (coffee, chocolate, mints, wine, spicy/citrus foods), but it is not always helpful to eliminate all these types of foods (American Gastroenterological Association 2008). If the patient has a clear pattern of reflux from a specific food type however, they should consider avoiding that and/or using treatment, per Dr. Oxentenko. Tobacco and alcohol reduction does not necessarily improve pH readings (Kaltenbach 2006), despite general health benefits from cessation.
Refractory GERD: The Reflux Strikes Back
If a patient continues to have reflux symptoms despite PPI use, then lifestyle, medication compliance, time of administration, and dose should be assessed. Switching to another PPI or increasing to twice a day may be considered in adherent patients, per Dr. Oxentenko. Adding a nighttime H2 blocker can be beneficial in patients with breakthrough nocturnal symptoms initially but unfortunately, they tend to lose that benefit overtime due to tachyphylaxis. Severe refractory GERD after PPI therapy requires an endoscopic investigation and, if that is inconclusive, a pH and/or impedance study, per Dr. Oxentenko.
Dyspepsia
Patients with dyspepsia feature pain as their predominant symptom (Talley 2016). They may have associated symptoms such as nausea, heartburn or bloating, but pain is their primary complaint. Functional dyspepsia has two subtypes based on the pattern of symptoms 1) epigastric pain syndrome and 2) postprandial distress syndrome.
DYSPEPSIA ALGORITHM
It is not feasible or practical to perform upper endoscopy for all patients with dyspepsia. Therefore, the 2017 AGS guidelines recommend against endoscopy for those under 60 yo even if they have one alarm symptom (Moayyedi 2017) since <1% of patients will have a serious finding . A more reasonable approach is to screen for H. pylori and treat patients if positive. Patient can be given a PPI trial if H. pylori testing is negative. The AGS guidelines recommend endoscopy for patients >60 yo with new onset symptoms given a higher risk of malignant findings. Dr. Oxentenko points out that these are guidelines and the decision to pursue testing and treatment should take into account patient factors and red flag symptoms (see below). She also reminds us to look for lifestyle factors or medications, such as NSAID or opioid use, that could be causing symptoms.
Red flag symptoms (Talley 2015)
- age >55 with new onset dyspepsia (Note: New AGS guidelines raised age to 60 yo —Moayyedi 2017)
- GI bleeding
- Dysphagia
- Persistent vomiting
- Weight loss
- Family history of GI cancer
- Palpable abdominal or epigastric mass
- Iron deficiency anemia
MORE ON H. PYLORI
H. pylori infection should be ruled out (in patients from high prevalence areas) via urease breath test or a stool antigen test (Talley 2015). Dr. Oxentenko prefers stool antigen testing over the urea breath test which can have false negatives from factors such as recent antibiotic use. Note: Talley et al note it is more practical to pursue H. pylori testing for most patients with dyspepsia since the local prevalence is often unknown to the treating provider and testing is noninvasive and inexpensive.
FUNCTIONAL DYSPEPSIA TREATMENT BY SUBTYPE
Patients may be started on a time-limited course of once-daily PPI if H. pylori screening is negative. If there is no symptomatic relief, the next line options are tricyclic antidepressants (TCAs) or prokinetic agents (e.g. metoclopramide). Note: Dr. Oxentenko, warns that the risk and side effect profiles of prokinetic agents make them unfavorable since they require monitoring for problems such as tardive dyskinesia, which can be irreversible. Patients with epigastric pain syndrome tend to benefit more from a TCA (ie: amitriptyline) (Talley 2015). In patients with postprandial distress syndrome, buspirone may assist with stomach relaxation, per Dr. Oxentenko. A GI psychologist or cognitive behavioral therapist may help if all else fails. Some patients find STW 5 beneficial, but some studies show hepatotoxicity as a potential adverse effect (Sáez-González 2016).